Dudley Strategy for Tackling Health Inequalities 2010-15
Dudley Strategy for Tackling Health Inequalities 2010-15
Dudley Strategy for Tackling Health Inequalities 2010-15
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
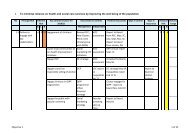
7. PRIORITY ACTIONS TO IMPACT ON HEALTH INEQUALITIESBuilding on its experience of supporting the spearhead areas to reduce healthinequalities, the <strong>Health</strong> <strong>Inequalities</strong> National Support Team has been able to developa number of priority actions that have been shown to have the greatest impact onmortality targets. Their recommendations <strong>for</strong> <strong>Dudley</strong> included a number of importantactions <strong>for</strong> us to implement in order to address our inequality gap. This sectionfocuses on the key disease areas that contribute to the biggest gaps locally.7.1 SECONDARY PREVENTION CARDIO-VASCULAR DISEASEIntroduction:Cardiovascular Disease (CVD) is a collective term <strong>for</strong> a group of related conditionsaffecting the heart, arteries or blood vessels. It includes Coronary Heart Disease(CHD) (about 50%) and stroke (about 25%).Nationally there has been a steady and marked decline in death rates from CVD. Infact the overall reduction has surpassed the government target:„substantially reduce mortality rates by <strong>2010</strong> from heart disease and stroke andrelated diseases by at least 40% in people under 75, with a 40% reduction in theinequalities gap between the fifth of areas with the worst health and deprivationindicators and the population as a whole from a 1996/7 baseline‟.The health inequalities gap in relation to CVD mortality and prevalence is welldocumented with higher levels <strong>for</strong> men than women, lower income levels than higherand <strong>for</strong> specific ethnic groups. Deaths from CHD are three times higher amongunskilled men than professionals and around 50% higher in South Asiancommunities than the general population and early onset of the disease two to threetimes higher (CQC, 2009).Nationally the CVD inequalities gap is reducing, with latest data (2007) showing areduction of 36% in the absolute gap between the Spearhead PCTs and the Englandaverage. The national gap in 2007 was 23.5 deaths/100,000. (CQC, 2009, p. 12).<strong>Dudley</strong> reflects the national picture overall but our inequalities gap is widening <strong>for</strong>men. CVD levels have declined steadily, but remain the biggest single cause ofpremature death in <strong>Dudley</strong> accounting <strong>for</strong> around <strong>15</strong>0 deaths in the under 75s eachyear. There is some evidence that <strong>for</strong> men the rate of decline is beginning to slow.CVD continues to be a major factor in overall health inequalities, with rates in somewards being more than 3 times those in other wards. The gap between the wardswith the highest and lowest rates has widened <strong>for</strong> men but not <strong>for</strong> women. Thedeprivation gradient in premature mortality from circulatory diseases is much steeperin men than in women. (Little and Moss, 2009)61