Dudley Strategy for Tackling Health Inequalities 2010-15
Dudley Strategy for Tackling Health Inequalities 2010-15
Dudley Strategy for Tackling Health Inequalities 2010-15
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
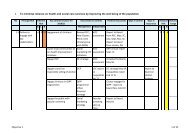
7.2 ACUTE CARDIO-VASCULAR DISEASE (CVD), TRANSIENT ISCHAEMICATTACK (TIA) AND STROKEThis section focuses on the priority areas of acute care <strong>for</strong> CHD, specifically acutemyocardial infarction (AMI) or heart attack, TIA and stroke.Coronary Heart Disease (CHD)A heart attack is said to have occurred when the myocardium (heart muscle) isdamaged as a result of impaired blood supply. This is known as a myocardialinfarction. The amount of damage is greatest when the blood supply to part of theheart is cut off altogether as a result of a thrombus (blood clot <strong>for</strong>mation) within oneof the coronary arteries (blood vessels) supplying that area of the heart. Under thesecircumstances, the electrocardiogram (ECG) recorded after the onset of occlusionwill usually show an abnormality termed „ST elevation‟. Patients suffering from thiscondition are said to have sustained „ST elevation myocardial infarction‟, abbreviatedto STEMI and require emergency reperfusion treatment with either thrombolyticdrugs or, the preferred option, primary percutaneous coronary intervention (PCI) byangioplasty and stenting, aiming to treat within 1 hour of the onset of symptoms.Non-ST elevation myocardial infarction or NSTEMI does not require very rapidemergency reperfusion treatment, but does require specialist cardiologyinvolvement, access to angiography and coronary intervention in the <strong>for</strong>m of drugs orrevascularisation. STEMI accounts <strong>for</strong> approximately 40% and NSTEMI 60% of allMIs, although the number of STEMI is falling and NSTEMI remaining static (MINAP,2009).Establishing the level of health equity involves investigating if differences exist inaccess and treatment/ treatment outcomes based on deprivation, ethnicity, age, sexand occupation. The extent to which this can be achieved easily depends on thelevel of data available especially within routine data sets and also thecoverage/reach of a service or programme. Routine hospital activity data has beenused to examine equity of access, treatment/treatment outcomes. Areas reviewedinclude:AdmissionsTotal admissions <strong>for</strong> CVDAdmissions, and access to diagnostics and interventional treatment <strong>for</strong>acute myocardial infarction( AMI)Secondary Prevention Prescribing <strong>for</strong> AMICardiac rehabilitationTotal admissions <strong>for</strong> all CVD increased by a small but statistically significant amount<strong>for</strong> the 3 year rate (2006/7-2008/9) This increase was due to an increase in electiveadmissions, particularly <strong>for</strong> women. (Figure 1). Emergency admissions remainedconstant. (Figure 2). All increases relate to hypertension admissions both electiveand emergency particularly <strong>for</strong> men and also to elective diabetes admissionsparticularly <strong>for</strong> women. The admissions data <strong>for</strong> CVD and AMI shows that at themacro level, admissions generally reflected the higher risk and needs of specific74