

Pathology of the Head and Neck
Pathology of the Head and Neck
Pathology of the Head and Neck
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
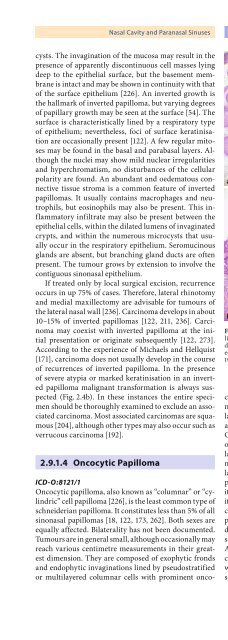
Nasal Cavity <strong>and</strong> Paranasal Sinuses Chapter 2 47cysts. The invagination <strong>of</strong> <strong>the</strong> mucosa may result in <strong>the</strong>presence <strong>of</strong> apparently discontinuous cell masses lyingdeep to <strong>the</strong> epi<strong>the</strong>lial surface, but <strong>the</strong> basement membraneis intact <strong>and</strong> may be shown in continuity with that<strong>of</strong> <strong>the</strong> surface epi<strong>the</strong>lium [226]. An inverted growth is<strong>the</strong> hallmark <strong>of</strong> inverted papilloma, but varying degrees<strong>of</strong> papillary growth may be seen at <strong>the</strong> surface [54]. Thesurface is characteristically lined by a respiratory type<strong>of</strong> epi<strong>the</strong>lium; never<strong>the</strong>less, foci <strong>of</strong> surface keratinisationare occasionally present [122]. A few regular mitosesmay be found in <strong>the</strong> basal <strong>and</strong> parabasal layers. Although<strong>the</strong> nuclei may show mild nuclear irregularities<strong>and</strong> hyperchromatism, no disturbances <strong>of</strong> <strong>the</strong> cellularpolarity are found. An abundant <strong>and</strong> oedematous connectivetissue stroma is a common feature <strong>of</strong> invertedpapillomas. It usually contains macrophages <strong>and</strong> neutrophils,but eosinophils may also be present. This inflammatoryinfiltrate may also be present between <strong>the</strong>epi<strong>the</strong>lial cells, within <strong>the</strong> dilated lumens <strong>of</strong> invaginatedcrypts, <strong>and</strong> within <strong>the</strong> numerous microcysts that usuallyoccur in <strong>the</strong> respiratory epi<strong>the</strong>lium. Seromucinousgl<strong>and</strong>s are absent, but branching gl<strong>and</strong> ducts are <strong>of</strong>tenpresent. The tumour grows by extension to involve <strong>the</strong>contiguous sinonasal epi<strong>the</strong>lium.If treated only by local surgical excision, recurrenceoccurs in up 75% <strong>of</strong> cases. Therefore, lateral rhinotomy<strong>and</strong> medial maxillectomy are advisable for tumours <strong>of</strong><strong>the</strong> lateral nasal wall [236]. Carcinoma develops in about10–15% <strong>of</strong> inverted papillomas [122, 211, 236]. Carcinomamay coexist with inverted papilloma at <strong>the</strong> initialpresentation or originate subsequently [122, 273].According to <strong>the</strong> experience <strong>of</strong> Michaels <strong>and</strong> Hellquist[171], carcinoma does not usually develop in <strong>the</strong> course<strong>of</strong> recurrences <strong>of</strong> inverted papilloma. In <strong>the</strong> presence<strong>of</strong> severe atypia or marked keratinisation in an invertedpapilloma malignant transformation is always suspected(Fig. 2.4b). In <strong>the</strong>se instances <strong>the</strong> entire specimenshould be thoroughly examined to exclude an associatedcarcinoma. Most associated carcinomas are squamous[204], although o<strong>the</strong>r types may also occur such asverrucous carcinoma [192].2.9.1.4 Oncocytic PapillomaabFig. 2.4. a Inverted papilloma: prominent invaginating cryptslined by hyperplastic respiratory epi<strong>the</strong>lium are supported by oedematousconnective tissue. b Squamous cell carcinoma ex invertedpapilloma: remnants <strong>of</strong> benign invaginating crypts are seen betweeninvasive cords <strong>of</strong> squamous epi<strong>the</strong>liumICD-O:8121/1Oncocytic papilloma, also known as “columnar” or “cylindric”cell papilloma [226], is <strong>the</strong> least common type <strong>of</strong>schneiderian papilloma. It constitutes less than 5% <strong>of</strong> allsinonasal papillomas [18, 122, 173, 262]. Both sexes areequally affected. Bilaterality has not been documented.Tumours are in general small, although occasionally mayreach various centimetre measurements in <strong>the</strong>ir greatestdimension. They are composed <strong>of</strong> exophytic fronds<strong>and</strong> endophytic invaginations lined by pseudostratifiedor multilayered columnar cells with prominent oncocyticfeatures. The cells have uniform hyperchromaticnuclei <strong>and</strong> abundant eosinophilic, occasionally granular,cytoplasm that contains abundant mitochondria<strong>and</strong> stains for <strong>the</strong> mitochondrial enzyme cytochromeC oxidase [59]. Goblet cells are not found. Cilia may beoccasionally encountered on <strong>the</strong> superficial epi<strong>the</strong>liallayer. Intraepi<strong>the</strong>lial microcysts containing mucin <strong>and</strong>neutrophils are usually present. These microcysts arelarger than <strong>the</strong> similar structures also seen in invertedpapilloma. The tumour resembles inverted papilloma inits sites <strong>of</strong> occurrence, <strong>the</strong> lateral wall <strong>of</strong> <strong>the</strong> nasal cavity<strong>and</strong> <strong>the</strong> maxillary antrum. The rate <strong>of</strong> recurrence isconsidered to be 36%, which is lower than in invertedpapilloma. The low frequency <strong>of</strong> this tumour makes itdifficult to evaluate its true malignant potential, whichseems to be similar to that <strong>of</strong> inverted papilloma [262].Atypical hyperplasia <strong>and</strong> carcinoma in situ changescan be occasionally found (Fig. 2.5). Surgical excisionwith wide margins is <strong>the</strong> treatment <strong>of</strong> choice. Invasivesquamous cell carcinoma, high-grade mucoepidermoid





