

Pathology of the Head and Neck
Pathology of the Head and Neck
Pathology of the Head and Neck
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
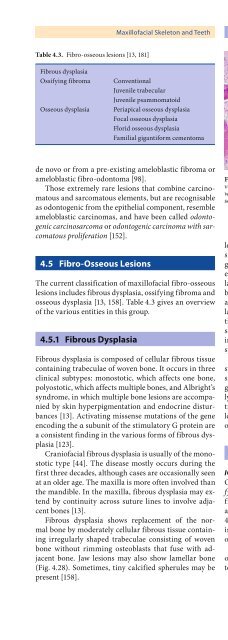
Maxill<strong>of</strong>acial Skeleton <strong>and</strong> Teeth Chapter 4 121Table 4.3. Fibro-osseous lesions [13, 181]Fibrous dysplasiaOssifying fibromaOsseous dysplasiaConventionalJuvenile trabecularJuvenile psammomatoidPeriapical osseous dysplasiaFocal osseous dysplasiaFlorid osseous dysplasiaFamilial gigantiform cementomade novo or from a pre-existing ameloblastic fibroma orameloblastic fibro-odontoma [98].Those extremely rare lesions that combine carcinomatous<strong>and</strong> sarcomatous elements, but are recognisableas odontogenic from <strong>the</strong> epi<strong>the</strong>lial component, resembleameloblastic carcinomas, <strong>and</strong> have been called odontogeniccarcinosarcoma or odontogenic carcinoma with sarcomatousproliferation [152].4.5 Fibro-Osseous LesionsThe current classification <strong>of</strong> maxill<strong>of</strong>acial fibro-osseouslesions includes fibrous dysplasia, ossifying fibroma <strong>and</strong>osseous dysplasia [13, 158]. Table 4.3 gives an overview<strong>of</strong> <strong>the</strong> various entities in this group.4.5.1 Fibrous DysplasiaFibrous dysplasia is composed <strong>of</strong> cellular fibrous tissuecontaining trabeculae <strong>of</strong> woven bone. It occurs in threeclinical subtypes: monostotic, which affects one bone,polyostotic, which affects multiple bones, <strong>and</strong> Albright’ssyndrome, in which multiple bone lesions are accompaniedby skin hyperpigmentation <strong>and</strong> endocrine disturbances[13]. Activating missense mutations <strong>of</strong> <strong>the</strong> geneencoding <strong>the</strong> α subunit <strong>of</strong> <strong>the</strong> stimulatory G protein area consistent finding in <strong>the</strong> various forms <strong>of</strong> fibrous dysplasia[123].Crani<strong>of</strong>acial fibrous dysplasia is usually <strong>of</strong> <strong>the</strong> monostotictype [44]. The disease mostly occurs during <strong>the</strong>first three decades, although cases are occasionally seenat an older age. The maxilla is more <strong>of</strong>ten involved than<strong>the</strong> m<strong>and</strong>ible. In <strong>the</strong> maxilla, fibrous dysplasia may extendby continuity across suture lines to involve adjacentbones [13].Fibrous dysplasia shows replacement <strong>of</strong> <strong>the</strong> normalbone by moderately cellular fibrous tissue containingirregularly shaped trabeculae consisting <strong>of</strong> wovenbone without rimming osteoblasts that fuse with adjacentbone. Jaw lesions may also show lamellar bone(Fig. 4.28). Sometimes, tiny calcified spherules may bepresent [158].Fig. 4.28. In <strong>the</strong> jaws, fibrous dysplasia may consist <strong>of</strong> both woven<strong>and</strong> lamellar bone, as shown in this photomicrograph takenwith <strong>the</strong> use <strong>of</strong> partly polarised light to enhance <strong>the</strong> collagenousscaffold <strong>of</strong> <strong>the</strong> boneFibrous dysplasia has to be distinguished from o<strong>the</strong>rlesions characterised by <strong>the</strong> combination <strong>of</strong> fibrous tissue<strong>and</strong> bone: ossifying fibroma, osseous dysplasia, lowgradeosteosarcoma <strong>and</strong> sclerosing osteomyelitis. However,none <strong>of</strong> <strong>the</strong>se is composed <strong>of</strong> woven bone trabeculaefusing with adjacent uninvolved bone. Ossifying fibroma<strong>and</strong> osseous dysplasia both show much variety inappearance <strong>of</strong> mineralised material <strong>and</strong> stromal cellularity,low-grade osteosarcoma invades through <strong>the</strong> corticalbone into s<strong>of</strong>t tissues <strong>and</strong> sclerosing osteomyelitisshows coarse trabeculae <strong>of</strong> lamellar bone, whereas <strong>the</strong>intervening stroma is not cellular but oedematous withsprinkled lymphocytes [158].Fibrous dysplasia clinically presents as a painlessswelling <strong>of</strong> <strong>the</strong> bone involved. Radiographically, <strong>the</strong> classicalappearance is described as orange-skin or groundglassradiopacity without defined borders [13]. Usually,fibrous dysplasia is a self-limiting disease. Therefore,treatment is only required if <strong>the</strong>re are problems due tolocal increase in size <strong>of</strong> <strong>the</strong> affected bone. Sometimes, anosteosarcoma may arise in fibrous dysplasia [39].4.5.2 Ossifying FibromaICD-O:9262/0, 9274/0Ossifying fibroma , formerly also called cemento-ossifyingfibroma is a well-demarcated lesion composed <strong>of</strong>fibrocellular tissue <strong>and</strong> mineralised material <strong>of</strong> varyingappearance. It occurs most <strong>of</strong>ten in <strong>the</strong> 2nd through <strong>the</strong>4th decades. The lesion shows a predilection for females,is mostly seen in <strong>the</strong> posterior m<strong>and</strong>ible [13] <strong>and</strong> mayoccur multifocally [70].Chromosomal abnormalities have been observed inossifying fibromas [31, 49, 138]. Data are still too scarceto determine <strong>the</strong>ir pathogenetic significance.





