

Pathology of the Head and Neck
Pathology of the Head and Neck
Pathology of the Head and Neck
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
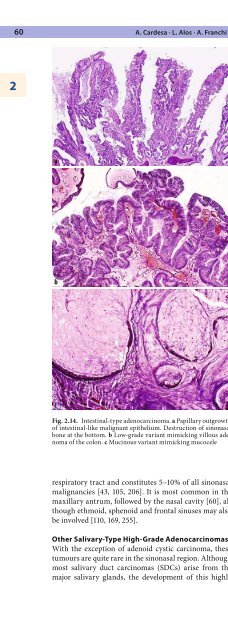
60 A. Cardesa · L. Alos · A. Franchi2aggressive tumour from <strong>the</strong> seromucous gl<strong>and</strong>s <strong>of</strong> <strong>the</strong>upper respiratory tract may occasionally occur. We haveseen one example <strong>of</strong> SDC originating in <strong>the</strong> maxillaryantrum, in which <strong>the</strong> characteristic ductal pattern, withcomedo-type necrosis, was only evident in <strong>the</strong> metastasesto <strong>the</strong> subm<strong>and</strong>ibular lymph nodes. The primarytumour was initially classified as adenocarcinoma noto<strong>the</strong>rwise specified (NOS) due to <strong>the</strong> absence <strong>of</strong> convincingdiagnostic features [40]. Carcinoma ex pleomorphicadenoma may also occur in <strong>the</strong> sinonasal tract [110].ab2.11.10 Low-Grade SinonasalAdenocarcinomasLow-grade adenocarcinomas arising primarily within<strong>the</strong> sinonasal tract are an uncommon <strong>and</strong> heterogeneousgroup <strong>of</strong> tumours [23, 113, 139, 150]. Some <strong>of</strong><strong>the</strong>se neoplasms show apparent histological continuitywith <strong>the</strong> normal surface epi<strong>the</strong>lium <strong>of</strong> <strong>the</strong> sinonasalmucosa, whereas o<strong>the</strong>rs are <strong>of</strong> salivary gl<strong>and</strong> origin. Allhave better prognosis <strong>and</strong> different clinical presentationthan <strong>the</strong>ir high-grade counterpart. With <strong>the</strong> exception<strong>of</strong> <strong>the</strong> well-differentiated, low-grade, adenocarcinomas<strong>of</strong> intestinal type, no correlation with occupational activitieshas been found in <strong>the</strong>se tumours.2.11.10.1 Non-Salivary-TypeLow-Grade AdenocarcinomascFig. 2.14. Intestinal-type adenocarcinoma. a Papillary outgrowth<strong>of</strong> intestinal-like malignant epi<strong>the</strong>lium. Destruction <strong>of</strong> sinonasalbone at <strong>the</strong> bottom. b Low-grade variant mimicking villous adenoma<strong>of</strong> <strong>the</strong> colon. c Mucinous variant mimicking mucocelerespiratory tract <strong>and</strong> constitutes 5–10% <strong>of</strong> all sinonasalmalignancies [43, 105, 206]. It is most common in <strong>the</strong>maxillary antrum, followed by <strong>the</strong> nasal cavity [60], althoughethmoid, sphenoid <strong>and</strong> frontal sinuses may alsobe involved [110, 169, 255].O<strong>the</strong>r Salivary-Type High-Grade AdenocarcinomasWith <strong>the</strong> exception <strong>of</strong> adenoid cystic carcinoma, <strong>the</strong>setumours are quite rare in <strong>the</strong> sinonasal region. Althoughmost salivary duct carcinomas (SDCs) arise from <strong>the</strong>major salivary gl<strong>and</strong>s, <strong>the</strong> development <strong>of</strong> this highlyNon-salivary-type low-grade sinonasal adenocarcinomasare a distinctive group <strong>of</strong> tumours comprising well-differentiatedtubular or papillary structures, or a combination<strong>of</strong> both. They are lined by a single layer <strong>of</strong> cuboidalor columnar cells that display uniform round or ovalnuclei, inconspicuous nucleoli, minimal cytologic atypia<strong>and</strong> scarce mitotic figures. They are locally infiltrative<strong>and</strong> have a tendency towards local recurrence [113].Different histological patterns may be recognised:papillary, gl<strong>and</strong>ular, mucinous, trabecular, cribriform<strong>and</strong> clear cell. The papillary pattern is characterised bycomplex papillary fronds lined by bl<strong>and</strong> columnar cellsthat may occasionally mimic oncocytic (columnar) cellpapilloma. Quite similar tumours also develop in <strong>the</strong>nasopharynx [267]. The gl<strong>and</strong>ular pattern may simulateadenoma; never<strong>the</strong>less, <strong>the</strong> presence <strong>of</strong> closely packedgl<strong>and</strong>s, forming back-to-back arrangements, indicates<strong>the</strong> true malignant nature. Mucinous tumours have to bedistinguished from mucoceles <strong>and</strong> from mucinous adenocarcinoma<strong>of</strong> intestinal or salivary type [20, 224]. Thetrabecular pattern may resemble acinic cell carcinoma[200]. The cribriform arrangements have to be distinguishedfrom low-grade salivary duct carcinoma <strong>of</strong> salivarygl<strong>and</strong>s [62]. The clear cell type has to be separatedfrom <strong>the</strong> salivary-type tumours with clear cells <strong>and</strong>





