

equity implications of health sector user fees in tanzania
equity implications of health sector user fees in tanzania
equity implications of health sector user fees in tanzania

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
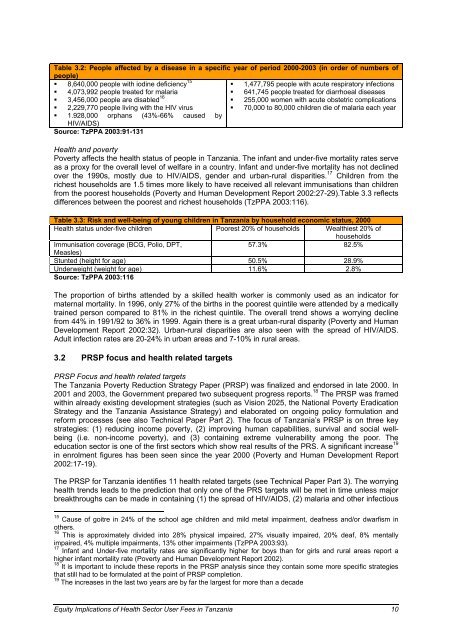
Table 3.2: People affected by a disease <strong>in</strong> a specific year <strong>of</strong> period 2000-2003 (<strong>in</strong> order <strong>of</strong> numbers <strong>of</strong><br />
people)<br />
� 8,640,000 people with iod<strong>in</strong>e deficiency 15<br />
�<br />
�<br />
4,073,992 people treated for malaria<br />
3,456,000 people are disabled 16<br />
� 2,229,770 people liv<strong>in</strong>g with the HIV virus<br />
� 1.928,000<br />
HIV/AIDS)<br />
orphans (43%-66% caused by<br />
Source: TzPPA 2003:91-131<br />
� 1,477,795 people with acute respiratory <strong>in</strong>fections<br />
� 641,745 people treated for diarrhoeal diseases<br />
� 255,000 women with acute obstetric complications<br />
� 70,000 to 80,000 children die <strong>of</strong> malaria each year<br />
Health and poverty<br />
Poverty affects the <strong>health</strong> status <strong>of</strong> people <strong>in</strong> Tanzania. The <strong>in</strong>fant and under-five mortality rates serve<br />
as a proxy for the overall level <strong>of</strong> welfare <strong>in</strong> a country. Infant and under-five mortality has not decl<strong>in</strong>ed<br />
over the 1990s, mostly due to HIV/AIDS, gender and urban-rural disparities. 17 Children from the<br />
richest households are 1.5 times more likely to have received all relevant immunisations than children<br />
from the poorest households (Poverty and Human Development Report 2002:27-29).Table 3.3 reflects<br />
differences between the poorest and richest households (TzPPA 2003:116).<br />
Table 3.3: Risk and well-be<strong>in</strong>g <strong>of</strong> young children <strong>in</strong> Tanzania by household economic status, 2000<br />
Health status under-five children Poorest 20% <strong>of</strong> households Wealthiest 20% <strong>of</strong><br />
households<br />
Immunisation coverage (BCG, Polio, DPT,<br />
57.3% 82.5%<br />
Measles)<br />
Stunted (height for age) 50.5% 28.9%<br />
Underweight (weight for age) 11.6% 2.8%<br />
Source: TzPPA 2003:116<br />
The proportion <strong>of</strong> births attended by a skilled <strong>health</strong> worker is commonly used as an <strong>in</strong>dicator for<br />
maternal mortality. In 1996, only 27% <strong>of</strong> the births <strong>in</strong> the poorest qu<strong>in</strong>tile were attended by a medically<br />
tra<strong>in</strong>ed person compared to 81% <strong>in</strong> the richest qu<strong>in</strong>tile. The overall trend shows a worry<strong>in</strong>g decl<strong>in</strong>e<br />
from 44% <strong>in</strong> 1991/92 to 36% <strong>in</strong> 1999. Aga<strong>in</strong> there is a great urban-rural disparity (Poverty and Human<br />
Development Report 2002:32). Urban-rural disparities are also seen with the spread <strong>of</strong> HIV/AIDS.<br />
Adult <strong>in</strong>fection rates are 20-24% <strong>in</strong> urban areas and 7-10% <strong>in</strong> rural areas.<br />
3.2 PRSP focus and <strong>health</strong> related targets<br />
PRSP Focus and <strong>health</strong> related targets<br />
The Tanzania Poverty Reduction Strategy Paper (PRSP) was f<strong>in</strong>alized and endorsed <strong>in</strong> late 2000. In<br />
2001 and 2003, the Government prepared two subsequent progress reports. 18 The PRSP was framed<br />
with<strong>in</strong> already exist<strong>in</strong>g development strategies (such as Vision 2025, the National Poverty Eradication<br />
Strategy and the Tanzania Assistance Strategy) and elaborated on ongo<strong>in</strong>g policy formulation and<br />
reform processes (see also Technical Paper Part 2). The focus <strong>of</strong> Tanzania’s PRSP is on three key<br />
strategies: (1) reduc<strong>in</strong>g <strong>in</strong>come poverty, (2) improv<strong>in</strong>g human capabilities, survival and social wellbe<strong>in</strong>g<br />
(i.e. non-<strong>in</strong>come poverty), and (3) conta<strong>in</strong><strong>in</strong>g extreme vulnerability among the poor. The<br />
education <strong>sector</strong> is one <strong>of</strong> the first <strong>sector</strong>s which show real results <strong>of</strong> the PRS. A significant <strong>in</strong>crease 19<br />
<strong>in</strong> enrolment figures has been seen s<strong>in</strong>ce the year 2000 (Poverty and Human Development Report<br />
2002:17-19).<br />
The PRSP for Tanzania identifies 11 <strong>health</strong> related targets (see Technical Paper Part 3). The worry<strong>in</strong>g<br />
<strong>health</strong> trends leads to the prediction that only one <strong>of</strong> the PRS targets will be met <strong>in</strong> time unless major<br />
breakthroughs can be made <strong>in</strong> conta<strong>in</strong><strong>in</strong>g (1) the spread <strong>of</strong> HIV/AIDS, (2) malaria and other <strong>in</strong>fectious<br />
15<br />
Cause <strong>of</strong> goitre <strong>in</strong> 24% <strong>of</strong> the school age children and mild metal impairment, deafness and/or dwarfism <strong>in</strong><br />
others.<br />
16<br />
This is approximately divided <strong>in</strong>to 28% physical impaired, 27% visually impaired, 20% deaf, 8% mentally<br />
impaired, 4% multiple impairments, 13% other impairments (TzPPA 2003:93).<br />
17<br />
Infant and Under-five mortality rates are significantly higher for boys than for girls and rural areas report a<br />
higher <strong>in</strong>fant mortality rate (Poverty and Human Development Report 2002).<br />
18<br />
It is important to <strong>in</strong>clude these reports <strong>in</strong> the PRSP analysis s<strong>in</strong>ce they conta<strong>in</strong> some more specific strategies<br />
that still had to be formulated at the po<strong>in</strong>t <strong>of</strong> PRSP completion.<br />
19<br />
The <strong>in</strong>creases <strong>in</strong> the last two years are by far the largest for more than a decade<br />
Equity Implications <strong>of</strong> Health Sector User Fees <strong>in</strong> Tanzania 10










