

equity implications of health sector user fees in tanzania
equity implications of health sector user fees in tanzania
equity implications of health sector user fees in tanzania

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
expectations. It appears that those who ultimately rema<strong>in</strong> <strong>in</strong> a pre-paid cost-shar<strong>in</strong>g scheme like the<br />
CHF are determ<strong>in</strong>ed by ‘adverse selection’, where people with greater <strong>health</strong> needs rema<strong>in</strong> <strong>in</strong> the<br />
CHF despite other dis<strong>in</strong>centives – like poor quality – to avoid high <strong>health</strong> care costs under the<br />
alternative <strong>fees</strong> for services. Bonu et al (2003) conclude that their f<strong>in</strong>d<strong>in</strong>gs suggest that the current<br />
CHF and <strong>user</strong> fee schemes <strong>in</strong> lower-level <strong>health</strong> facilities <strong>in</strong> Tanzania need to design effective built-<strong>in</strong><br />
mechanisms to protect women, the poor and elderly populations from adverse effects. Similar to<br />
decl<strong>in</strong><strong>in</strong>g <strong>in</strong>stitutional delivery rates observed among poor women after the <strong>in</strong>troduction <strong>of</strong> <strong>user</strong> <strong>fees</strong> <strong>in</strong><br />
higher level facilities, adverse effects might also be observed <strong>in</strong> primary <strong>health</strong> care for the poor on the<br />
<strong>in</strong>troduction <strong>of</strong> CHFs and <strong>user</strong> <strong>fees</strong> <strong>in</strong> lower-level facilities, unless accompanied by effective exemption<br />
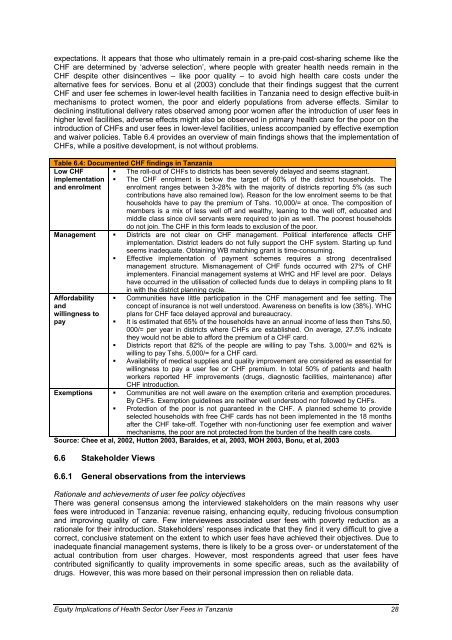
and waiver policies. Table 6.4 provides an overview <strong>of</strong> ma<strong>in</strong> f<strong>in</strong>d<strong>in</strong>gs shows that the implementation <strong>of</strong><br />
CHFs, while a positive development, is not without problems.<br />
Table 6.4: Documented CHF f<strong>in</strong>d<strong>in</strong>gs <strong>in</strong> Tanzania<br />
Low CHF<br />
implementation<br />
and enrolment<br />
Management<br />
Affordability<br />
and<br />
will<strong>in</strong>gness to<br />
pay<br />
� The roll-out <strong>of</strong> CHFs to districts has been severely delayed and seems stagnant.<br />
� The CHF enrolment is below the target <strong>of</strong> 60% <strong>of</strong> the district households. The<br />
enrolment ranges between 3-28% with the majority <strong>of</strong> districts report<strong>in</strong>g 5% (as such<br />
contributions have also rema<strong>in</strong>ed low). Reason for the low enrolment seems to be that<br />
households have to pay the premium <strong>of</strong> Tshs. 10,000/= at once. The composition <strong>of</strong><br />
members is a mix <strong>of</strong> less well <strong>of</strong>f and wealthy, lean<strong>in</strong>g to the well <strong>of</strong>f, educated and<br />
middle class s<strong>in</strong>ce civil servants were required to jo<strong>in</strong> as well. The poorest households<br />
do not jo<strong>in</strong>. The CHF <strong>in</strong> this form leads to exclusion <strong>of</strong> the poor.<br />
� Districts are not clear on CHF management. Political <strong>in</strong>terference affects CHF<br />
implementation. District leaders do not fully support the CHF system. Start<strong>in</strong>g up fund<br />
seems <strong>in</strong>adequate. Obta<strong>in</strong><strong>in</strong>g WB match<strong>in</strong>g grant is time-consum<strong>in</strong>g.<br />
� Effective implementation <strong>of</strong> payment schemes requires a strong decentralised<br />
management structure. Mismanagement <strong>of</strong> CHF funds occurred with 27% <strong>of</strong> CHF<br />
implementers. F<strong>in</strong>ancial management systems at WHC and HF level are poor. Delays<br />
have occurred <strong>in</strong> the utilisation <strong>of</strong> collected funds due to delays <strong>in</strong> compil<strong>in</strong>g plans to fit<br />
<strong>in</strong> with the district plann<strong>in</strong>g cycle.<br />
� Communities have little participation <strong>in</strong> the CHF management and fee sett<strong>in</strong>g. The<br />
concept <strong>of</strong> <strong>in</strong>surance is not well understood. Awareness on benefits is low (38%). WHC<br />
plans for CHF face delayed approval and bureaucracy.<br />
� It is estimated that 65% <strong>of</strong> the households have an annual <strong>in</strong>come <strong>of</strong> less then Tshs.50,<br />
000/= per year <strong>in</strong> districts where CHFs are established. On average, 27.5% <strong>in</strong>dicate<br />
they would not be able to afford the premium <strong>of</strong> a CHF card.<br />
� Districts report that 82% <strong>of</strong> the people are will<strong>in</strong>g to pay Tshs. 3,000/= and 62% is<br />
will<strong>in</strong>g to pay Tshs. 5,000/= for a CHF card.<br />
� Availability <strong>of</strong> medical supplies and quality improvement are considered as essential for<br />
will<strong>in</strong>gness to pay a <strong>user</strong> fee or CHF premium. In total 50% <strong>of</strong> patients and <strong>health</strong><br />
workers reported HF improvements (drugs, diagnostic facilities, ma<strong>in</strong>tenance) after<br />
CHF <strong>in</strong>troduction.<br />
Exemptions � Communities are not well aware on the exemption criteria and exemption procedures.<br />
By CHFs. Exemption guidel<strong>in</strong>es are neither well understood nor followed by CHFs.<br />
� Protection <strong>of</strong> the poor is not guaranteed <strong>in</strong> the CHF. A planned scheme to provide<br />
selected households with free CHF cards has not been implemented <strong>in</strong> the 18 months<br />
after the CHF take-<strong>of</strong>f. Together with non-function<strong>in</strong>g <strong>user</strong> fee exemption and waiver<br />
mechanisms, the poor are not protected from the burden <strong>of</strong> the <strong>health</strong> care costs.<br />
Source: Chee et al, 2002, Hutton 2003, Baraldes, et al, 2003, MOH 2003, Bonu, et al, 2003<br />
6.6 Stakeholder Views<br />
6.6.1 General observations from the <strong>in</strong>terviews<br />
Rationale and achievements <strong>of</strong> <strong>user</strong> fee policy objectives<br />
There was general consensus among the <strong>in</strong>terviewed stakeholders on the ma<strong>in</strong> reasons why <strong>user</strong><br />
<strong>fees</strong> were <strong>in</strong>troduced <strong>in</strong> Tanzania: revenue rais<strong>in</strong>g, enhanc<strong>in</strong>g <strong>equity</strong>, reduc<strong>in</strong>g frivolous consumption<br />
and improv<strong>in</strong>g quality <strong>of</strong> care. Few <strong>in</strong>terviewees associated <strong>user</strong> <strong>fees</strong> with poverty reduction as a<br />
rationale for their <strong>in</strong>troduction. Stakeholders’ responses <strong>in</strong>dicate that they f<strong>in</strong>d it very difficult to give a<br />
correct, conclusive statement on the extent to which <strong>user</strong> <strong>fees</strong> have achieved their objectives. Due to<br />
<strong>in</strong>adequate f<strong>in</strong>ancial management systems, there is likely to be a gross over- or understatement <strong>of</strong> the<br />
actual contribution from <strong>user</strong> charges. However, most respondents agreed that <strong>user</strong> <strong>fees</strong> have<br />
contributed significantly to quality improvements <strong>in</strong> some specific areas, such as the availability <strong>of</strong><br />
drugs. However, this was more based on their personal impression then on reliable data.<br />
Equity Implications <strong>of</strong> Health Sector User Fees <strong>in</strong> Tanzania 28










