

equity implications of health sector user fees in tanzania
equity implications of health sector user fees in tanzania
equity implications of health sector user fees in tanzania

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
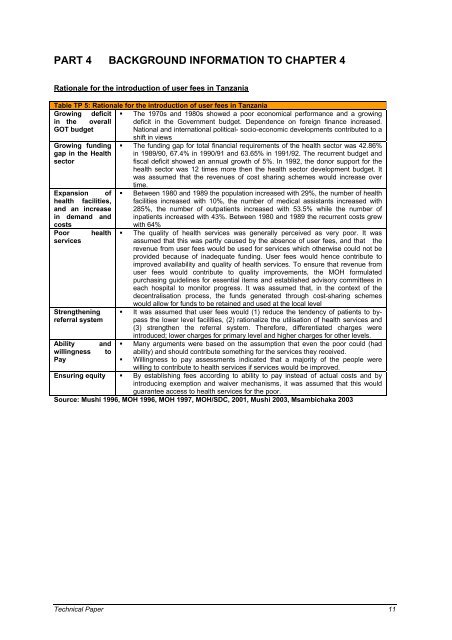
PART 4 BACKGROUND INFORMATION TO CHAPTER 4<br />
Rationale for the <strong>in</strong>troduction <strong>of</strong> <strong>user</strong> <strong>fees</strong> <strong>in</strong> Tanzania<br />
Table TP 5: Rationale for the <strong>in</strong>troduction <strong>of</strong> <strong>user</strong> <strong>fees</strong> <strong>in</strong> Tanzania<br />
Grow<strong>in</strong>g deficit<br />
<strong>in</strong> the overall<br />
GOT budget<br />
Grow<strong>in</strong>g fund<strong>in</strong>g<br />
gap <strong>in</strong> the Health<br />
<strong>sector</strong><br />
Expansion <strong>of</strong><br />
<strong>health</strong> facilities,<br />
and an <strong>in</strong>crease<br />
<strong>in</strong> demand and<br />
costs<br />
Poor <strong>health</strong><br />
services<br />
Strengthen<strong>in</strong>g<br />
referral system<br />
Ability and<br />
will<strong>in</strong>gness to<br />
Pay<br />
� The 1970s and 1980s showed a poor economical performance and a grow<strong>in</strong>g<br />
deficit <strong>in</strong> the Government budget. Dependence on foreign f<strong>in</strong>ance <strong>in</strong>creased.<br />
National and <strong>in</strong>ternational political- socio-economic developments contributed to a<br />
shift <strong>in</strong> views<br />
� The fund<strong>in</strong>g gap for total f<strong>in</strong>ancial requirements <strong>of</strong> the <strong>health</strong> <strong>sector</strong> was 42.86%<br />
<strong>in</strong> 1989/90, 67.4% <strong>in</strong> 1990/91 and 63.65% <strong>in</strong> 1991/92. The recurrent budget and<br />
fiscal deficit showed an annual growth <strong>of</strong> 5%. In 1992, the donor support for the<br />
<strong>health</strong> <strong>sector</strong> was 12 times more then the <strong>health</strong> <strong>sector</strong> development budget. It<br />
was assumed that the revenues <strong>of</strong> cost shar<strong>in</strong>g schemes would <strong>in</strong>crease over<br />
time.<br />
� Between 1980 and 1989 the population <strong>in</strong>creased with 29%, the number <strong>of</strong> <strong>health</strong><br />
facilities <strong>in</strong>creased with 10%, the number <strong>of</strong> medical assistants <strong>in</strong>creased with<br />
285%, the number <strong>of</strong> outpatients <strong>in</strong>creased with 53.5% while the number <strong>of</strong><br />
<strong>in</strong>patients <strong>in</strong>creased with 43%. Between 1980 and 1989 the recurrent costs grew<br />
with 64%<br />
� The quality <strong>of</strong> <strong>health</strong> services was generally perceived as very poor. It was<br />
assumed that this was partly caused by the absence <strong>of</strong> <strong>user</strong> <strong>fees</strong>, and that the<br />
revenue from <strong>user</strong> <strong>fees</strong> would be used for services which otherwise could not be<br />
provided because <strong>of</strong> <strong>in</strong>adequate fund<strong>in</strong>g. User <strong>fees</strong> would hence contribute to<br />
improved availability and quality <strong>of</strong> <strong>health</strong> services. To ensure that revenue from<br />
<strong>user</strong> <strong>fees</strong> would contribute to quality improvements, the MOH formulated<br />
purchas<strong>in</strong>g guidel<strong>in</strong>es for essential items and established advisory committees <strong>in</strong><br />
each hospital to monitor progress. It was assumed that, <strong>in</strong> the context <strong>of</strong> the<br />
decentralisation process, the funds generated through cost-shar<strong>in</strong>g schemes<br />
would allow for funds to be reta<strong>in</strong>ed and used at the local level<br />
� It was assumed that <strong>user</strong> <strong>fees</strong> would (1) reduce the tendency <strong>of</strong> patients to bypass<br />
the lower level facilities, (2) rationalize the utilisation <strong>of</strong> <strong>health</strong> services and<br />
(3) strengthen the referral system. Therefore, differentiated charges were<br />
<strong>in</strong>troduced; lower charges for primary level and higher charges for other levels.<br />
� Many arguments were based on the assumption that even the poor could (had<br />
ability) and should contribute someth<strong>in</strong>g for the services they received.<br />
� Will<strong>in</strong>gness to pay assessments <strong>in</strong>dicated that a majority <strong>of</strong> the people were<br />
will<strong>in</strong>g to contribute to <strong>health</strong> services if services would be improved.<br />
Ensur<strong>in</strong>g <strong>equity</strong> � By establish<strong>in</strong>g <strong>fees</strong> accord<strong>in</strong>g to ability to pay <strong>in</strong>stead <strong>of</strong> actual costs and by<br />
<strong>in</strong>troduc<strong>in</strong>g exemption and waiver mechanisms, it was assumed that this would<br />
guarantee access to <strong>health</strong> services for the poor.<br />
Source: Mushi 1996, MOH 1996, MOH 1997, MOH/SDC, 2001, Mushi 2003, Msambichaka 2003<br />
Technical Paper 11










