

equity implications of health sector user fees in tanzania
equity implications of health sector user fees in tanzania
equity implications of health sector user fees in tanzania

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
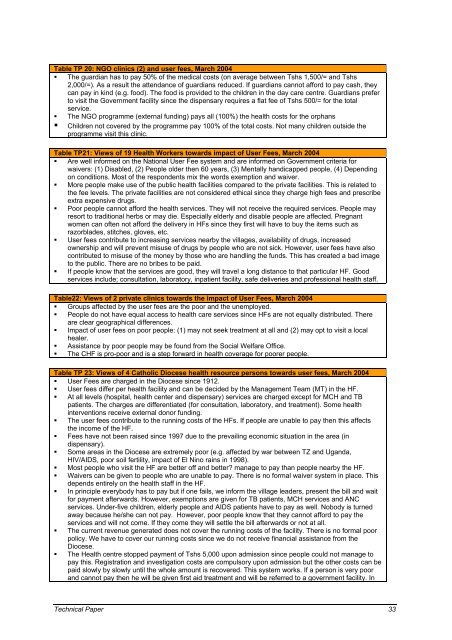
Table TP 20: NGO cl<strong>in</strong>ics (2) and <strong>user</strong> <strong>fees</strong>, March 2004<br />
� The guardian has to pay 50% <strong>of</strong> the medical costs (on average between Tshs 1,500/= and Tshs<br />
2,000/=). As a result the attendance <strong>of</strong> guardians reduced. If guardians cannot afford to pay cash, they<br />
can pay <strong>in</strong> k<strong>in</strong>d (e.g. food). The food is provided to the children <strong>in</strong> the day care centre. Guardians prefer<br />
to visit the Government facility s<strong>in</strong>ce the dispensary requires a flat fee <strong>of</strong> Tshs 500/= for the total<br />
service.<br />
� The NGO programme (external fund<strong>in</strong>g) pays all (100%) the <strong>health</strong> costs for the orphans<br />
� Children not covered by the programme pay 100% <strong>of</strong> the total costs. Not many children outside the<br />
programme visit this cl<strong>in</strong>ic.<br />
Table TP21: Views <strong>of</strong> 19 Health Workers towards impact <strong>of</strong> User Fees, March 2004<br />
� Are well <strong>in</strong>formed on the National User Fee system and are <strong>in</strong>formed on Government criteria for<br />
waivers: (1) Disabled, (2) People older then 60 years, (3) Mentally handicapped people, (4) Depend<strong>in</strong>g<br />
on conditions. Most <strong>of</strong> the respondents mix the words exemption and waiver.<br />
� More people make use <strong>of</strong> the public <strong>health</strong> facilities compared to the private facilities. This is related to<br />
the fee levels. The private facilities are not considered ethical s<strong>in</strong>ce they charge high <strong>fees</strong> and prescribe<br />
extra expensive drugs.<br />
� Poor people cannot afford the <strong>health</strong> services. They will not receive the required services. People may<br />
resort to traditional herbs or may die. Especially elderly and disable people are affected. Pregnant<br />
women can <strong>of</strong>ten not afford the delivery <strong>in</strong> HFs s<strong>in</strong>ce they first will have to buy the items such as<br />
razorblades, stitches, gloves, etc.<br />
� User <strong>fees</strong> contribute to <strong>in</strong>creas<strong>in</strong>g services nearby the villages, availability <strong>of</strong> drugs, <strong>in</strong>creased<br />
ownership and will prevent misuse <strong>of</strong> drugs by people who are not sick. However, <strong>user</strong> <strong>fees</strong> have also<br />
contributed to misuse <strong>of</strong> the money by those who are handl<strong>in</strong>g the funds. This has created a bad image<br />
to the public. There are no bribes to be paid.<br />
� If people know that the services are good, they will travel a long distance to that particular HF. Good<br />
services <strong>in</strong>clude; consultation, laboratory, <strong>in</strong>patient facility, safe deliveries and pr<strong>of</strong>essional <strong>health</strong> staff.<br />
Table22: Views <strong>of</strong> 2 private cl<strong>in</strong>ics towards the impact <strong>of</strong> User Fees, March 2004<br />
� Groups affected by the <strong>user</strong> <strong>fees</strong> are the poor and the unemployed.<br />
� People do not have equal access to <strong>health</strong> care services s<strong>in</strong>ce HFs are not equally distributed. There<br />
are clear geographical differences.<br />
� Impact <strong>of</strong> <strong>user</strong> <strong>fees</strong> on poor people: (1) may not seek treatment at all and (2) may opt to visit a local<br />
healer.<br />
� Assistance by poor people may be found from the Social Welfare Office.<br />
� The CHF is pro-poor and is a step forward <strong>in</strong> <strong>health</strong> coverage for poorer people.<br />
Table TP 23: Views <strong>of</strong> 4 Catholic Diocese <strong>health</strong> resource persons towards <strong>user</strong> <strong>fees</strong>, March 2004<br />
� User Fees are charged <strong>in</strong> the Diocese s<strong>in</strong>ce 1912.<br />
� User <strong>fees</strong> differ per <strong>health</strong> facility and can be decided by the Management Team (MT) <strong>in</strong> the HF.<br />
� At all levels (hospital, <strong>health</strong> center and dispensary) services are charged except for MCH and TB<br />
patients. The charges are differentiated (for consultation, laboratory, and treatment). Some <strong>health</strong><br />
<strong>in</strong>terventions receive external donor fund<strong>in</strong>g.<br />
� The <strong>user</strong> <strong>fees</strong> contribute to the runn<strong>in</strong>g costs <strong>of</strong> the HFs. If people are unable to pay then this affects<br />
the <strong>in</strong>come <strong>of</strong> the HF.<br />
� Fees have not been raised s<strong>in</strong>ce 1997 due to the prevail<strong>in</strong>g economic situation <strong>in</strong> the area (<strong>in</strong><br />
dispensary).<br />
� Some areas <strong>in</strong> the Diocese are extremely poor (e.g. affected by war between TZ and Uganda,<br />
HIV/AIDS, poor soil fertility, impact <strong>of</strong> El N<strong>in</strong>o ra<strong>in</strong>s <strong>in</strong> 1998).<br />
� Most people who visit the HF are better <strong>of</strong>f and better? manage to pay than people nearby the HF.<br />
� Waivers can be given to people who are unable to pay. There is no formal waiver system <strong>in</strong> place. This<br />
depends entirely on the <strong>health</strong> staff <strong>in</strong> the HF.<br />
� In pr<strong>in</strong>ciple everybody has to pay but if one fails, we <strong>in</strong>form the village leaders, present the bill and wait<br />
for payment afterwards. However, exemptions are given for TB patients, MCH services and ANC<br />
services. Under-five children, elderly people and AIDS patients have to pay as well. Nobody is turned<br />
away because he/she can not pay. However, poor people know that they cannot afford to pay the<br />
services and will not come. If they come they will settle the bill afterwards or not at all.<br />
� The current revenue generated does not cover the runn<strong>in</strong>g costs <strong>of</strong> the facility. There is no formal poor<br />
policy. We have to cover our runn<strong>in</strong>g costs s<strong>in</strong>ce we do not receive f<strong>in</strong>ancial assistance from the<br />
Diocese.<br />
� The Health centre stopped payment <strong>of</strong> Tshs 5,000 upon admission s<strong>in</strong>ce people could not manage to<br />
pay this. Registration and <strong>in</strong>vestigation costs are compulsory upon admission but the other costs can be<br />
paid slowly by slowly until the whole amount is recovered. This system works. If a person is very poor<br />
and cannot pay then he will be given first aid treatment and will be referred to a government facility. In<br />
Technical Paper 33










