Lockout / Tagout - Ohio Bureau of Workers' Compensation
Lockout / Tagout - Ohio Bureau of Workers' Compensation
Lockout / Tagout - Ohio Bureau of Workers' Compensation

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
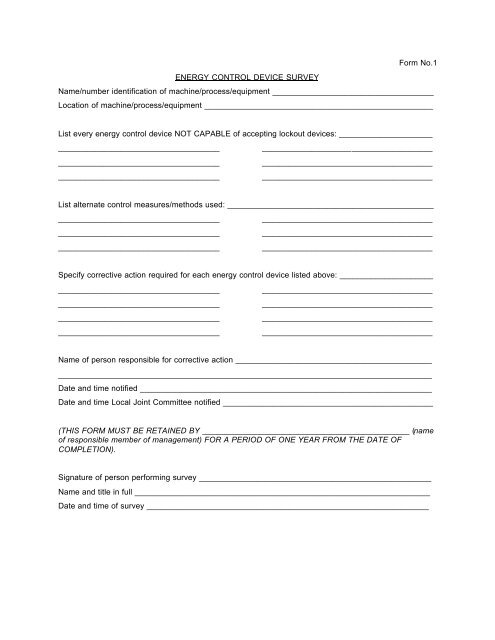
Form No.1<br />
ENERGY CONTROL DEVICE SURVEY<br />
Name/number identification <strong>of</strong> machine/process/equipment ____________________________________<br />
Location <strong>of</strong> machine/process/equipment ___________________________________________________<br />
List every energy control device NOT CAPABLE <strong>of</strong> accepting lockout devices: _____________________<br />
____________________________________<br />
______________________________________<br />
____________________________________<br />
______________________________________<br />
____________________________________<br />
______________________________________<br />
List alternate control measures/methods used: ______________________________________________<br />
____________________________________<br />
______________________________________<br />
____________________________________<br />
______________________________________<br />
____________________________________<br />
______________________________________<br />
Specify corrective action required for each energy control device listed above: _____________________<br />
____________________________________<br />
____________________________________<br />
____________________________________<br />
____________________________________<br />
______________________________________<br />
______________________________________<br />
______________________________________<br />
______________________________________<br />
Name <strong>of</strong> person responsible for corrective action ____________________________________________<br />
___________________________________________________________________________________<br />
Date and time notified _________________________________________________________________<br />
Date and time Local Joint Committee notified _______________________________________________<br />
(THIS FORM MUST BE RETAINED BY ______________________________________________ (name<br />
<strong>of</strong> responsible member <strong>of</strong> management) FOR A PERIOD OF ONE YEAR FROM THE DATE OF<br />
COMPLETION).<br />
Signature <strong>of</strong> person performing survey ____________________________________________________<br />
Name and title in full __________________________________________________________________<br />
Date and time <strong>of</strong> survey _______________________________________________________________