Lockout / Tagout - Ohio Bureau of Workers' Compensation
Lockout / Tagout - Ohio Bureau of Workers' Compensation
Lockout / Tagout - Ohio Bureau of Workers' Compensation

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
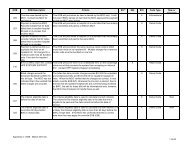
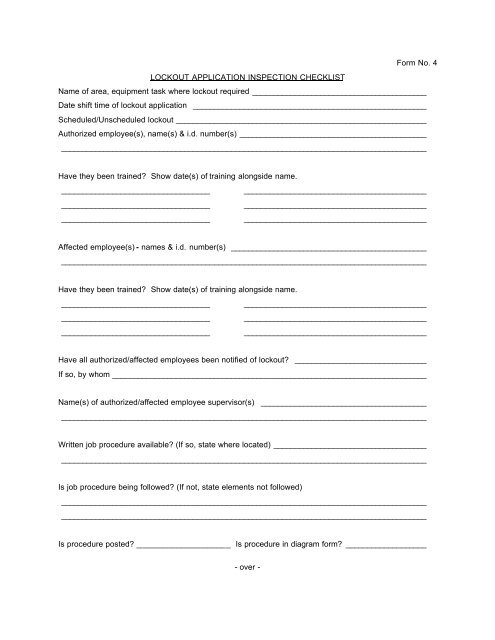
Form No. 4<br />
LOCKOUT APPLICATION INSPECTION CHECKLIST<br />
Name <strong>of</strong> area, equipment task where lockout required _________________________________________<br />
Date shift time <strong>of</strong> lockout application _______________________________________________________<br />
Scheduled/Unscheduled lockout ___________________________________________________________<br />
Authorized employee(s), name(s) & i.d. number(s) ____________________________________________<br />
______________________________________________________________________________________<br />
Have they been trained? Show date(s) <strong>of</strong> training alongside name.<br />
___________________________________ ___________________________________________<br />
___________________________________ ___________________________________________<br />
___________________________________ ___________________________________________<br />
Affected employee(s) - names & i.d. number(s) ______________________________________________<br />
______________________________________________________________________________________<br />
Have they been trained? Show date(s) <strong>of</strong> training alongside name.<br />
___________________________________ ___________________________________________<br />
___________________________________ ___________________________________________<br />
___________________________________ ___________________________________________<br />
Have all authorized/affected employees been notified <strong>of</strong> lockout? _______________________________<br />
If so, by whom __________________________________________________________________________<br />
Name(s) <strong>of</strong> authorized/affected employee supervisor(s) _______________________________________<br />
______________________________________________________________________________________<br />
Written job procedure available? (If so, state where located) ____________________________________<br />
______________________________________________________________________________________<br />
Is job procedure being followed? (If not, state elements not followed)<br />
______________________________________________________________________________________<br />
______________________________________________________________________________________<br />
Is procedure posted? _____________________ Is procedure in diagram form? ___________________<br />
- over -