Lockout / Tagout - Ohio Bureau of Workers' Compensation
Lockout / Tagout - Ohio Bureau of Workers' Compensation
Lockout / Tagout - Ohio Bureau of Workers' Compensation

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
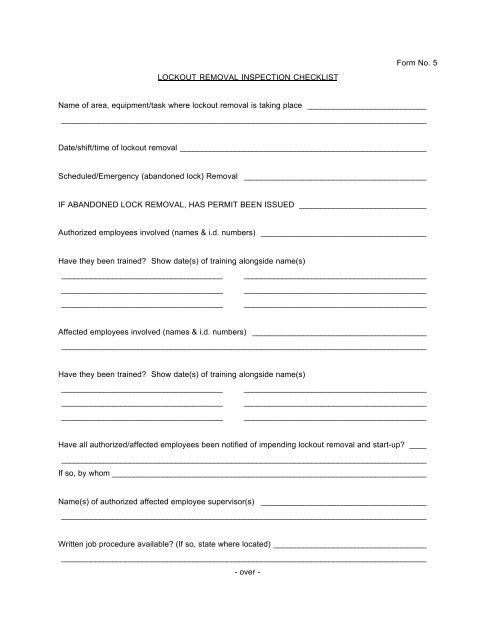
Form No. 5<br />
LOCKOUT REMOVAL INSPECTION CHECKLIST<br />
Name <strong>of</strong> area, equipment/task where lockout removal is taking place ____________________________<br />
______________________________________________________________________________________<br />
Date/shift/time <strong>of</strong> lockout removal __________________________________________________________<br />
Scheduled/Emergency (abandoned lock) Removal ___________________________________________<br />
IF ABANDONED LOCK REMOVAL, HAS PERMIT BEEN ISSUED ______________________________<br />
Authorized employees involved (names & i.d. numbers) _______________________________________<br />
Have they been trained? Show date(s) <strong>of</strong> training alongside name(s)<br />
______________________________________ ___________________________________________<br />
______________________________________ ___________________________________________<br />
______________________________________ ___________________________________________<br />
Affected employees involved (names & i.d. numbers) _________________________________________<br />
______________________________________________________________________________________<br />
Have they been trained? Show date(s) <strong>of</strong> training alongside name(s)<br />
______________________________________ ___________________________________________<br />
______________________________________ ___________________________________________<br />
______________________________________ ___________________________________________<br />
Have all authorized/affected employees been notified <strong>of</strong> impending lockout removal and start-up? ____<br />
______________________________________________________________________________________<br />
If so, by whom __________________________________________________________________________<br />
Name(s) <strong>of</strong> authorized affected employee supervisor(s) _______________________________________<br />
______________________________________________________________________________________<br />
Written job procedure available? (If so, state where located) ____________________________________<br />
______________________________________________________________________________________<br />
- over -