Lockout / Tagout - Ohio Bureau of Workers' Compensation
Lockout / Tagout - Ohio Bureau of Workers' Compensation
Lockout / Tagout - Ohio Bureau of Workers' Compensation

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
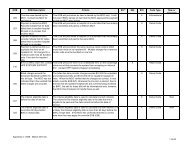
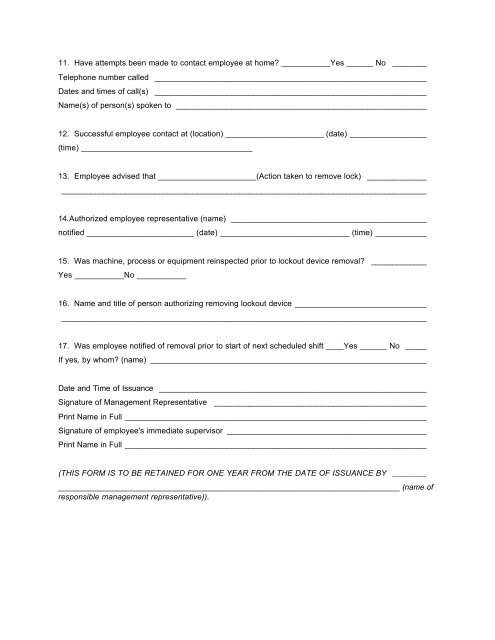
11. Have attempts been made to contact employee at home? ___________Yes ______ No ________<br />
Telephone number called ________________________________________________________________<br />
Dates and times <strong>of</strong> call(s) ________________________________________________________________<br />
Name(s) <strong>of</strong> person(s) spoken to ___________________________________________________________<br />
12. Successful employee contact at (location) ______________________ (date) __________________<br />
(time) ______________________________________<br />
13. Employee advised that ______________________(Action taken to remove lock) ______________<br />
______________________________________________________________________________________<br />
14.Authorized employee representative (name) ______________________________________________<br />
notified ________________________ (date) _____________________________ (time) ____________<br />
15. Was machine, process or equipment reinspected prior to lockout device removal? _____________<br />
Yes ___________No ___________<br />
16. Name and title <strong>of</strong> person authorizing removing lockout device _______________________________<br />
______________________________________________________________________________________<br />
17. Was employee notified <strong>of</strong> removal prior to start <strong>of</strong> next scheduled shift ____Yes ______ No _____<br />
If yes, by whom? (name) _________________________________________________________________<br />
Date and Time <strong>of</strong> Issuance _______________________________________________________________<br />
Signature <strong>of</strong> Management Representative __________________________________________________<br />
Print Name in Full _______________________________________________________________________<br />
Signature <strong>of</strong> employee's immediate supervisor _______________________________________________<br />
Print Name in Full _______________________________________________________________________<br />
(THIS FORM IS TO BE RETAINED FOR ONE YEAR FROM THE DATE OF ISSUANCE BY ________<br />
____________________________________________________________________________ (name <strong>of</strong><br />
responsible management representative)).