Lockout / Tagout - Ohio Bureau of Workers' Compensation
Lockout / Tagout - Ohio Bureau of Workers' Compensation
Lockout / Tagout - Ohio Bureau of Workers' Compensation

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
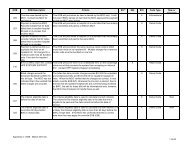
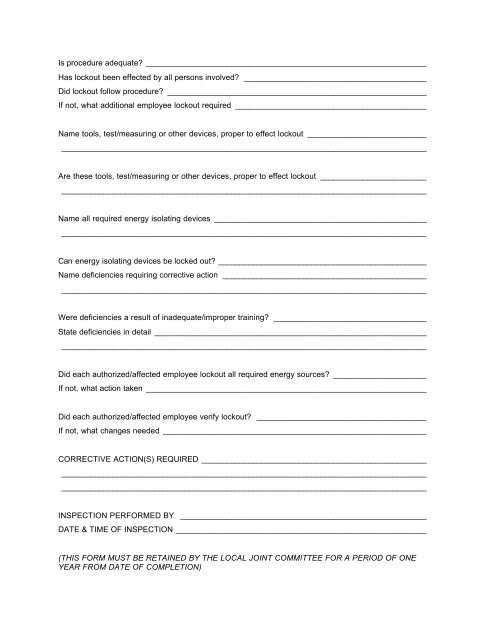
Is procedure adequate? __________________________________________________________________<br />
Has lockout been effected by all persons involved? ___________________________________________<br />
Did lockout follow procedure? _____________________________________________________________<br />
If not, what additional employee lockout required _____________________________________________<br />
Name tools, test/measuring or other devices, proper to effect lockout ____________________________<br />
______________________________________________________________________________________<br />
Are these tools, test/measuring or other devices, proper to effect lockout _________________________<br />
______________________________________________________________________________________<br />
Name all required energy isolating devices __________________________________________________<br />
______________________________________________________________________________________<br />
Can energy isolating devices be locked out? _________________________________________________<br />
Name deficiencies requiring corrective action ________________________________________________<br />
______________________________________________________________________________________<br />
Were deficiencies a result <strong>of</strong> inadequate/improper training? ____________________________________<br />
State deficiencies in detail ________________________________________________________________<br />
______________________________________________________________________________________<br />
Did each authorized/affected employee lockout all required energy sources? ______________________<br />
If not, what action taken __________________________________________________________________<br />
Did each authorized/affected employee verify lockout? ________________________________________<br />
If not, what changes needed ______________________________________________________________<br />
CORRECTIVE ACTION(S) REQUIRED _____________________________________________________<br />
______________________________________________________________________________________<br />
______________________________________________________________________________________<br />
INSPECTION PERFORMED BY __________________________________________________________<br />
DATE & TIME OF INSPECTION ___________________________________________________________<br />
(THIS FORM MUST BE RETAINED BY THE LOCAL JOINT COMMITTEE FOR A PERIOD OF ONE<br />
YEAR FROM DATE OF COMPLETION)