State of World Population 2012 - Country Page List - UNFPA
State of World Population 2012 - Country Page List - UNFPA
State of World Population 2012 - Country Page List - UNFPA

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
pregnancy, their inability to negotiate contraceptive<br />
use with their (usually older) husbands, or<br />
to access services contribute to high levels <strong>of</strong><br />
childbearing in adolescence.<br />
Few family planning programmes include<br />
strategies for reaching child brides who are <strong>of</strong>ten<br />
isolated, without well-developed social networks,<br />
and vulnerable to many adverse maternal health<br />
outcomes associated with early pregnancy and<br />
childbirth. This is another important area for<br />
investment. (Malhotra et al., 2011; Bruce and<br />
Clark, 2003; <strong>UNFPA</strong>, 2009; Lloyd, 2009;<br />
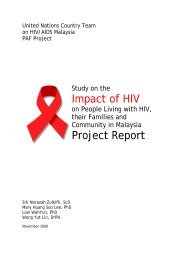
Countries with the highest<br />
rates <strong>of</strong> child marriage<br />
<strong>Country</strong><br />
Per cent girls<br />
married before<br />
age 18<br />
Niger 75%<br />
Chad 72%<br />
Bangladesh 66%<br />
Guinea 63%<br />
Central African Republic 61%<br />
Mali 55%<br />
Mozambique 52%<br />
Malawi 50%<br />
Madagascar 48%<br />
Sierra Leone 48%<br />
Burkina Faso 48%<br />
India 47%<br />
Eritrea 47%<br />
Uganda 46%<br />
Somalia 45%<br />
Nicaragua 43%<br />
Zambia 42%<br />
Ethiopia 41%<br />
Nepal 41%<br />
Dominican Republic 40%<br />
Source: <strong>UNFPA</strong>, <strong>2012</strong><br />
<strong>World</strong> Health Organization, 2008; Lam,<br />
Marteleto and Ranchhod, 2009; Levine et al,<br />
2008; Mensch, Bruce and Greene, 1999.)<br />
Poor quality as an obstacle to family<br />
planning use<br />
When services are unreliable or delivered by<br />
untrained personnel, or when a full range <strong>of</strong><br />
contraceptives and information is unavailable,<br />
people with unmet need may choose not to take<br />
advantage <strong>of</strong> family planning and are therefore<br />
unable to exercise their right to it.<br />
Health systems in many countries struggle to<br />
meet the challenge <strong>of</strong> managing their human<br />
resources effectively, making sure that infrastructure<br />
is adequate to the task <strong>of</strong> providing services<br />
and ensuring the supply <strong>of</strong> adequate materials<br />
and equipment <strong>of</strong> all kinds. People living in<br />
rural areas are especially vulnerable to weaknesses<br />
in the health system that can leave them beyond<br />
the reach <strong>of</strong> services available to people in towns<br />
and cities.<br />
One consequence <strong>of</strong> poor guidance on a rightsbased<br />
approach to health and weak management<br />
<strong>of</strong> staff can be the biased and discriminatory<br />
attitudes <strong>of</strong> health workers. Some providers internalize<br />
social biases towards minority populations.<br />
Health workers’ attitudes can affect the quality <strong>of</strong><br />
information given to specific clients, resulting in<br />
a lack <strong>of</strong> informed choice and options.<br />
A lack <strong>of</strong> privacy and inability to communicate<br />
are barriers to service delivery for some<br />
groups. A recent multi-country study found that<br />
health programmes in refugee camps did not<br />
ensure the right to privacy, confidentiality, and<br />
non-discrimination to all, particularly for adolescents<br />
and unmarried persons (United Nations<br />
High Commissioner for Refugees, 2011). In<br />
some settings, internally displaced persons or<br />
refugees are <strong>of</strong>ten unable to access quality services<br />
due to limited commitment to helping<br />
66 CHAPTER 3: CHALLENGES IN EXTENDING ACCESS TO EVERYONE