

Het volume van chirurgische ingrepen en de impact ervan op ... - KCE
Het volume van chirurgische ingrepen en de impact ervan op ... - KCE
Het volume van chirurgische ingrepen en de impact ervan op ... - KCE

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>KCE</strong> Reports 113 Volume Outcome 151<br />
RELATION BETWEEN SURGEON VOLUME AND MORTALITY RATE<br />
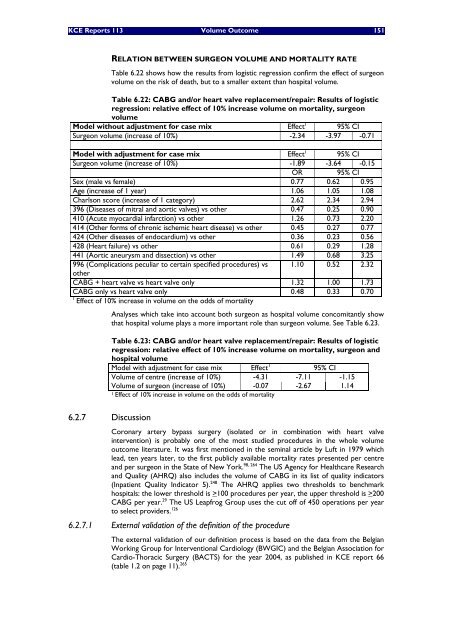
Table 6.22 shows how the results from logistic regression confirm the effect of surgeon<br />
<strong>volume</strong> on the risk of <strong>de</strong>ath, but to a smaller ext<strong>en</strong>t than hospital <strong>volume</strong>.<br />
Table 6.22: CABG and/or heart valve replacem<strong>en</strong>t/repair: Results of logistic<br />
regression: relative effect of 10% increase <strong>volume</strong> on mortality, surgeon<br />
<strong>volume</strong><br />
Mo<strong>de</strong>l without adjustm<strong>en</strong>t for case mix Effect 1 95% CI<br />
Surgeon <strong>volume</strong> (increase of 10%) -2.34 -3.97 -0.71<br />
Mo<strong>de</strong>l with adjustm<strong>en</strong>t for case mix Effect 1 95% CI<br />
Surgeon <strong>volume</strong> (increase of 10%) -1.89 -3.64 -0.15<br />
OR 95% CI<br />
Sex (male vs female) 0.77 0.62 0.95<br />
Age (increase of 1 year) 1.06 1.05 1.08<br />
Charlson score (increase of 1 category) 2.62 2.34 2.94<br />
396 (Diseases of mitral and aortic valves) vs other 0.47 0.25 0.90<br />
410 (Acute myocardial infarction) vs other 1.26 0.73 2.20<br />
414 (Other forms of chronic ischemic heart disease) vs other 0.45 0.27 0.77<br />
424 (Other diseases of <strong>en</strong>docardium) vs other 0.36 0.23 0.56<br />
428 (Heart failure) vs other 0.61 0.29 1.28<br />
441 (Aortic aneurysm and dissection) vs other 1.49 0.68 3.25<br />
996 (Complications peculiar to certain specified procedures) vs 1.10 0.52 2.32<br />
other<br />
CABG + heart valve vs heart valve only 1.32 1.00 1.73<br />
CABG only vs heart valve only 0.48 0.33 0.70<br />
1 Effect of 10% increase in <strong>volume</strong> on the odds of mortality<br />
6.2.7 Discussion<br />
Analyses which take into account both surgeon as hospital <strong>volume</strong> concomitantly show<br />
that hospital <strong>volume</strong> plays a more important role than surgeon <strong>volume</strong>. See Table 6.23.<br />
Table 6.23: CABG and/or heart valve replacem<strong>en</strong>t/repair: Results of logistic<br />
regression: relative effect of 10% increase <strong>volume</strong> on mortality, surgeon and<br />
hospital <strong>volume</strong><br />
Mo<strong>de</strong>l with adjustm<strong>en</strong>t for case mix Effect 1 95% CI<br />
Volume of c<strong>en</strong>tre (increase of 10%) -4.31 -7.11 -1.15<br />
Volume of surgeon (increase of 10%) -0.07 -2.67 1.14<br />
1 Effect of 10% increase in <strong>volume</strong> on the odds of mortality<br />
Coronary artery bypass surgery (isolated or in combination with heart valve<br />
interv<strong>en</strong>tion) is probably one of the most studied procedures in the whole <strong>volume</strong><br />
outcome literature. It was first m<strong>en</strong>tioned in the seminal article by Luft in 1979 which<br />
lead, t<strong>en</strong> years later, to the first publicly available mortality rates pres<strong>en</strong>ted per c<strong>en</strong>tre<br />
and per surgeon in the State of New York. 98, 264 The US Ag<strong>en</strong>cy for Healthcare Research<br />
and Quality (AHRQ) also inclu<strong>de</strong>s the <strong>volume</strong> of CABG in its list of quality indicators<br />
(Inpati<strong>en</strong>t Quality Indicator 5). 248 The AHRQ applies two thresholds to b<strong>en</strong>chmark<br />
hospitals: the lower threshold is >100 procedures per year, the upper threshold is >200<br />
CABG per year. 29 The US Leapfrog Group uses the cut off of 450 <strong>op</strong>erations per year<br />
to select provi<strong>de</strong>rs. 126<br />
6.2.7.1 External validation of the <strong>de</strong>finition of the procedure<br />
The external validation of our <strong>de</strong>finition process is based on the data from the Belgian<br />
Working Group for Interv<strong>en</strong>tional Cardiology (BWGIC) and the Belgian Association for<br />
Cardio-Thoracic Surgery (BACTS) for the year 2004, as published in <strong>KCE</strong> report 66<br />
(table 1.2 on page 11). 265














