

Primary Retinal Detachment
Primary Retinal Detachment
Primary Retinal Detachment

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Are Encircling and Drainage Still Worth Doing? 47<br />
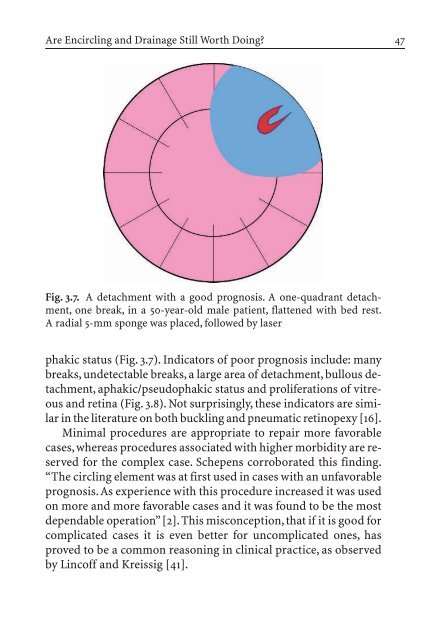
Fig. 3.7. A detachment with a good prognosis. A one-quadrant detachment,<br />
one break, in a 50-year-old male patient, flattened with bed rest.<br />
A radial 5-mm sponge was placed, followed by laser<br />
phakic status (Fig. 3.7). Indicators of poor prognosis include: many<br />
breaks, undetectable breaks, a large area of detachment, bullous detachment,<br />
aphakic/pseudophakic status and proliferations of vitreous<br />
and retina (Fig. 3.8). Not surprisingly, these indicators are similar<br />
in the literature on both buckling and pneumatic retinopexy [16].<br />
Minimal procedures are appropriate to repair more favorable<br />
cases, whereas procedures associated with higher morbidity are reserved<br />
for the complex case. Schepens corroborated this finding.<br />
“The circling element was at first used in cases with an unfavorable<br />
prognosis.As experience with this procedure increased it was used<br />
on more and more favorable cases and it was found to be the most<br />
dependable operation”[2]. This misconception, that if it is good for<br />
complicated cases it is even better for uncomplicated ones, has<br />
proved to be a common reasoning in clinical practice, as observed<br />
by Lincoff and Kreissig [41].


