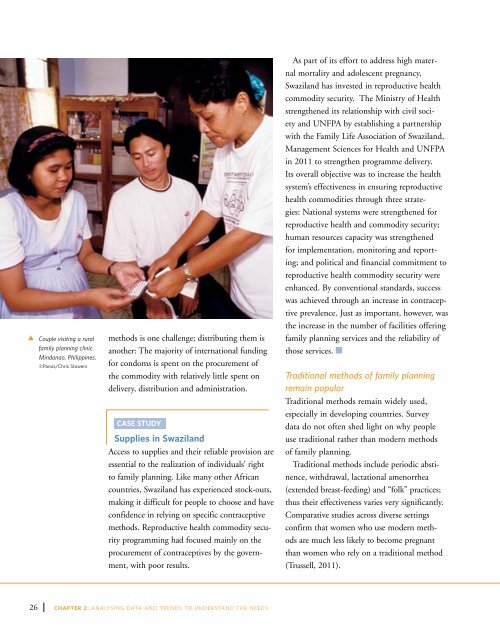
tCouple visiting a ruralfamily planning clinic.Mindanao, Philippines.©Panos/Chris Stowersmethods is one challenge; distributing them isanother: The majority <strong>of</strong> international fundingfor condoms is spent on the procurement <strong>of</strong>the commodity with relatively little spent ondelivery, distribution and administration.CASE STUDYSupplies in SwazilandAccess to supplies and their reliable provision areessential to the realization <strong>of</strong> individuals’ rightto family planning. Like many other Africancountries, Swaziland has experienced stock-outs,making it difficult for people to choose and haveconfidence in relying on specific contraceptivemethods. Reproductive health commodity securityprogramming had focused mainly on theprocurement <strong>of</strong> contraceptives by the government,with poor results.As part <strong>of</strong> its effort to address high maternalmortality and adolescent pregnancy,Swaziland has invested in reproductive healthcommodity security. The Ministry <strong>of</strong> Healthstrengthened its relationship with civil societyand <strong>UNFPA</strong> by establishing a partnershipwith the Family Life Association <strong>of</strong> Swaziland,Management Sciences for Health and <strong>UNFPA</strong>in 2011 to strengthen programme delivery.Its overall objective was to increase the healthsystem’s effectiveness in ensuring reproductivehealth commodities through three strategies:National systems were strengthened forreproductive health and commodity security;human resources capacity was strengthenedfor implementation, monitoring and reporting;and political and financial commitment toreproductive health commodity security wereenhanced. By conventional standards, successwas achieved through an increase in contraceptiveprevalence. Just as important, however, wasthe increase in the number <strong>of</strong> facilities <strong>of</strong>feringfamily planning services and the reliability <strong>of</strong>those services.Traditional methods <strong>of</strong> family planningremain popularTraditional methods remain widely used,especially in developing countries. Surveydata do not <strong>of</strong>ten shed light on why peopleuse traditional rather than modern methods<strong>of</strong> family planning.Traditional methods include periodic abstinence,withdrawal, lactational amenorrhea(extended breast-feeding) and “folk” practices;thus their effectiveness varies very significantly.Comparative studies across diverse settingsconfirm that women who use modern methodsare much less likely to become pregnantthan women who rely on a traditional method(Trussell, 2011).26 CHAPTER 2: ANALYSING DATA AND TRENDS TO UNDERSTAND THE needs
Despite the tendency to consolidate all traditionalmethods into a singular category, notall traditional methods are the same. Severalcountries have good histories with non-modern,traditional methods. For example, withdrawalis a commonly used among educated couplesin Iran and Turkey and has been widely usedto prevent pregnancy in Sicily and Pakistan(Cottingham, Germain and Hunt, <strong>2012</strong>; Erfani,2010). The Demographic and Health Surveyscategorize coitus interruptus as a “totally ineffectivefolk method,” even though this method isused extensively in a number <strong>of</strong> countries andis about as effective as condoms (Cottingham,Germain and Hunt, <strong>2012</strong>).five married women. Nearly everywhere, womenare far more likely to undergo the sterilizationprocedure than men. In Colombia, for example,where 78 per cent <strong>of</strong> women are current contraceptiveusers, nearly a third <strong>of</strong> all women(31 per cent) have been sterilized, comparedwith just two per cent <strong>of</strong> men (United Nations,Department <strong>of</strong> Economic and Social Affairs,2011). Since desired fertility declines over time,couples married at young ages will stop havingchildren at earlier ages. After reaching theirdesired fertility, these younger couples may haveto avoid unintended pregnancy for up to 25years, making permanent methods attractiveto them.Female methods <strong>of</strong> family planning morewidely used than male methodsThe ICPD Programme <strong>of</strong> Action noted as a“high priority… the development <strong>of</strong> new methodsfor the regulation <strong>of</strong> fertility for men,” andcalled for the involvement <strong>of</strong> private industry.It urged countries to take special efforts toenhance male involvement and responsibilityin family planning (Paragraph 12.14.). Nearly20 years later, no new male methods have beenwidely introduced to the public. With few contraceptiveoptions for men, men’s use <strong>of</strong> familyplanning has been less than envisioned by theICPD. Today, even if all traditional methodsrequiring men’s cooperation (rhythm, withdrawaland others) are counted together withmale condoms, male methods account for about26 per cent <strong>of</strong> global contraceptive prevalence(United Nations, Department <strong>of</strong> Economic andSocial Affairs, 2011).Female sterilization rates far outnumber malerates. Although the decision to permanently endchildbearing can be difficult, sterilization is themost commonly used family planning methodin the world, relied upon by more than one in”Although the decision to permanently end childbearing canbe difficult, sterilization is the most commonly used familyplanning method in the world, relied upon by more than onein five married women.”While female sterilization rates are highest inLatin and Central America, ranging as high as47 per cent in the Dominican Republic, only 14countries in the world have at least 5 per cent<strong>of</strong> men who have undergone vasectomy. Maleand female sterilization rates are most similar inAustralia and New Zealand, where about 15 percent <strong>of</strong> both men and women have been sterilized(United Nations, Department <strong>of</strong> Economicand Social Affairs, 2011). Male sterilizationexceeds female sterilization in only a handful<strong>of</strong> countries, most notably in Canada and theUnited Kingdom, where men are about twice aslikely as women to be sterilized.One might infer from the mostly developedcountries that vasectomy rates primarily reflectwomen’s economic power and rights in thesecountries. Nepal is among the few developingcountries where vasectomy rates are aboveTHE STATE OF WORLD POPULATION <strong>2012</strong>27
- Page 6 and 7: OverviewOne hundred seventy-nine go
- Page 8 and 9: The report is structured to answer
- Page 10 and 11: viiiCHAPTER 1: THE RIGHT TO FAMILY
- Page 12 and 13: “All human beings are born free a
- Page 14 and 15: Treaties, conventions and agreement
- Page 16 and 17: Health: a social and economic right
- Page 18: “Everyone has the right to educat
- Page 21 and 22: designing and delivering accessible
- Page 23 and 24: use, and reduces unintended pregnan
- Page 26 and 27: 16 CHAPTER 2: ANALYSING DATA AND TR
- Page 28 and 29: Change in Age-Specific Fertility Ra
- Page 30 and 31: Sexuality, sexual and gender stereo
- Page 32 and 33: not necessarily associated with a d
- Page 34 and 35: METHOD EFFECTIVENESSMethod, rankedf
- Page 38: Demand and supply over time5 per ce
- Page 41 and 42: contribute to high unmet need (Sing
- Page 43 and 44: abortions in the region lead to mor
- Page 45 and 46: (as stated in the Convention on the
- Page 47 and 48: arriers prevent individuals from ac
- Page 49 and 50: CHAPTERTHREEChallenges in extending
- Page 51 and 52: sources of sexual and reproductive
- Page 53 and 54: messages were delivered via a numbe
- Page 55 and 56: Ricardo, 2005). Moreover, young and
- Page 58 and 59: per cent in Guatemala. Across all c
- Page 60 and 61: tTeenager inMadagascar listens toa
- Page 62 and 63: Consensual unions account for an in
- Page 64 and 65: when. The proportion of never-marri
- Page 66 and 67: 63 per cent to 93 per cent of young
- Page 68 and 69: Family planning in humanitariansett
- Page 71 and 72: Studies suggest that HIV may have a
- Page 73 and 74: with a public health challenge (Wor
- Page 75 and 76: State-run family planning programme
- Page 77 and 78: people in mobile, temporary, and re
- Page 79 and 80: systems and civic participation to
- Page 81 and 82: CHAPTERFOURThe social and economici
- Page 83 and 84: tCommunityeducation inCaracas, Vene
- Page 85 and 86: Estimates of Total Fertility2010-20
- Page 87 and 88:
children, and healthier women also
- Page 89 and 90:
empirical evidence supporting this
- Page 92 and 93:
tRicardo and Sarain Mexico City say
- Page 94 and 95:
to secure the future population’s
- Page 96 and 97:
86 CHAPTER 5: THE COSTS AND SAVINGS
- Page 98 and 99:
Unintended Pregnancies and outcomes
- Page 100 and 101:
tDonor Commitmentspanel at the Lond
- Page 102 and 103:
UNFPA supports the Health for All c
- Page 104 and 105:
tDr. BabatundeOsotimehin, Executive
- Page 106 and 107:
96 CHAPTER 6: MAKING THE RIGHT TO F
- Page 108 and 109:
When individuals are able to exerci
- Page 110 and 111:
Family planning programmes must ref
- Page 112 and 113:
Family planning programmes reinforc
- Page 114:
tPresident of NigeriaGoodluck Jonat
- Page 117 and 118:
Monitoring Monitoring ICPD ICPD Goa
- Page 119 and 120:
Monitoring Monitoring ICPD ICPD Goa
- Page 121 and 122:
Monitoring Monitoring ICPD ICPD Goa
- Page 123 and 124:
Monitoring ICPD Goals Demographic -
- Page 125 and 126:
Monitoring ICPD Goals - Selected In
- Page 127 and 128:
BibliographyAbbasi-Shavazi, Mohamma
- Page 129 and 130:
Monitoring ICPD Goals - Selected In
- Page 131 and 132:
Monitoring ICPD Goals - Selected In
- Page 133 and 134:
Monitoring ICPD Goals - Selected In
- Page 135 and 136:
Monitoring ICPD Goals - Selected In
- Page 137 and 138:
Monitoring ICPD Goals - Selected In
- Page 140:
Delivering a world where every preg