CASE STUDYExpanding family planning inhumanitarian settingsAs part <strong>of</strong> the emergency response in SouthSudan, <strong>UNFPA</strong> delivered supplies for oraland injectable contraception and insertion <strong>of</strong>intrauterine devices and other family planningcommodities (United Nations <strong>Population</strong>Fund, 2011a). And in collaboration withthe American Refugee Committee, <strong>UNFPA</strong>contributed to training health care workers,community distribution workers and peereducators on family planning.Strategies and programmes <strong>of</strong>ten fail to fulfilthe family planning needs <strong>of</strong> refugees and internallydisplaced populations who take refuge awayfrom home for varying lengths <strong>of</strong> time. A focuson the emergency provision <strong>of</strong> shelter, food, andbasic health services has not always includedtargeted programming to deliver essential reproductivehealth information and services. In recentyears however, humanitarian inter-agencyworking groups have developed resources andtools to help humanitarian personnel generatedemand for family planning and ensure refugees’right to family planning is met.Sex workers. Sex workers not only have a rightto time and space their children, but also to relyon condoms as a means <strong>of</strong> protecting themselvesfrom sexually transmitted infections includingHIV. However, sex workers <strong>of</strong>ten face socialstigma and discrimination, which subsequentlyinhibit them from accessing family planninginformation and services (Lin, 2007).Social norms <strong>of</strong>ten classify sex work as beingimmoral, and the institutions and individualsresponsible for law enforcement and healthmay reinforce discriminatory attitudes and practices,with harmful effects on sex workers. Forexample, in some countries such as Lebanonand the Philippines, stigma against sex work andnon-marital sex has been used to pass legislationthat prevents people from freely possessingcondoms (Human Rights Watch, 2004; <strong>World</strong>Health Organization, 2005). As a result, sexworkers <strong>of</strong>ten perceive that health systemsare non-responsive to their needs, includingdenying them access to the full range <strong>of</strong>available contraceptives.Studies affirm that when sex workers accessfamily planning services, they <strong>of</strong>ten do so reluctantlyand fall victim to the biases <strong>of</strong> health-careworkers who neglect their sexual and reproductivehealth needs, focusing primarily on the risk<strong>of</strong> HIV and sexually transmitted infections (Lin,2007; Human Rights Watch, 2004). There aredocumented cases <strong>of</strong> providers in South Asia andSouth East Asia being accused <strong>of</strong> exposing HIVstatuses and threatening to report those withHIV to the authorities (Mgbako et al., 2008).The consequences <strong>of</strong> the stigmatization <strong>of</strong>sex workers violate universal human rights.According to the <strong>World</strong> Health Organization,“interventions to promote safer sex among sexworkers must be part <strong>of</strong> an overall effort toensure their safety, promote their health andwell-being more broadly and protect their humanrights” (<strong>World</strong> Health Organization, 2005).Lesbian, gay, bisexual and transgenderedpeople. <strong>State</strong>-run family planning programmeslargely neglect the needs <strong>of</strong> those who identifythemselves as lesbian, gay, bisexual andtransgendered. The United Nations HighCommissioner for Human Rights has affirmedthat, “discrimination on the basis <strong>of</strong> sexualorientation is contrary to international humanrights law” (United Nations High Commissionerfor Human Rights, 2008). However, in mostplaces it is heterosexuals who are privileged in64 CHAPTER 3: CHALLENGES IN EXTENDING ACCESS TO EVERYONE
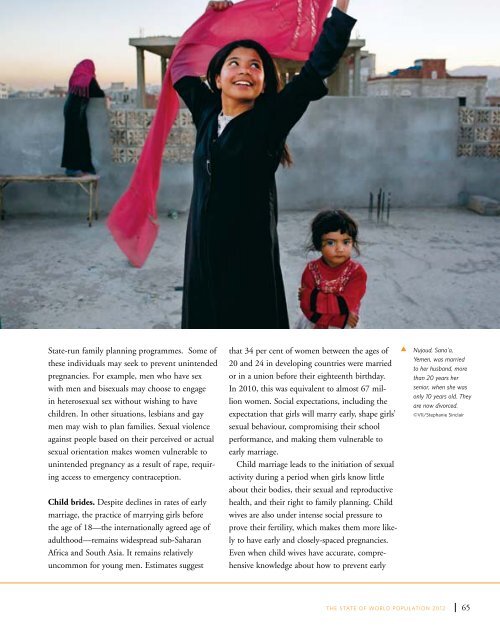
<strong>State</strong>-run family planning programmes. Some <strong>of</strong>these individuals may seek to prevent unintendedpregnancies. For example, men who have sexwith men and bisexuals may choose to engagein heterosexual sex without wishing to havechildren. In other situations, lesbians and gaymen may wish to plan families. Sexual violenceagainst people based on their perceived or actualsexual orientation makes women vulnerable tounintended pregnancy as a result <strong>of</strong> rape, requiringaccess to emergency contraception.Child brides. Despite declines in rates <strong>of</strong> earlymarriage, the practice <strong>of</strong> marrying girls beforethe age <strong>of</strong> 18—the internationally agreed age <strong>of</strong>adulthood—remains widespread sub-SaharanAfrica and South Asia. It remains relativelyuncommon for young men. Estimates suggestthat 34 per cent <strong>of</strong> women between the ages <strong>of</strong>20 and 24 in developing countries were marriedor in a union before their eighteenth birthday.In 2010, this was equivalent to almost 67 millionwomen. Social expectations, including theexpectation that girls will marry early, shape girls’sexual behaviour, compromising their schoolperformance, and making them vulnerable toearly marriage.Child marriage leads to the initiation <strong>of</strong> sexualactivity during a period when girls know littleabout their bodies, their sexual and reproductivehealth, and their right to family planning. Childwives are also under intense social pressure toprove their fertility, which makes them more likelyto have early and closely-spaced pregnancies.Even when child wives have accurate, comprehensiveknowledge about how to prevent earlytNujoud, Sana'a,Yemen, was marriedto her husband, morethan 20 years hersenior, when she wasonly 10 years old. Theyare now divorced.©VII/Stephanie SinclairTHE STATE OF WORLD POPULATION <strong>2012</strong>65
- Page 6 and 7:
OverviewOne hundred seventy-nine go
- Page 8 and 9:
The report is structured to answer
- Page 10 and 11:
viiiCHAPTER 1: THE RIGHT TO FAMILY
- Page 12 and 13:
“All human beings are born free a
- Page 14 and 15:
Treaties, conventions and agreement
- Page 16 and 17:
Health: a social and economic right
- Page 18:
“Everyone has the right to educat
- Page 21 and 22:
designing and delivering accessible
- Page 23 and 24: use, and reduces unintended pregnan
- Page 26 and 27: 16 CHAPTER 2: ANALYSING DATA AND TR
- Page 28 and 29: Change in Age-Specific Fertility Ra
- Page 30 and 31: Sexuality, sexual and gender stereo
- Page 32 and 33: not necessarily associated with a d
- Page 34 and 35: METHOD EFFECTIVENESSMethod, rankedf
- Page 36 and 37: tCouple visiting a ruralfamily plan
- Page 38: Demand and supply over time5 per ce
- Page 41 and 42: contribute to high unmet need (Sing
- Page 43 and 44: abortions in the region lead to mor
- Page 45 and 46: (as stated in the Convention on the
- Page 47 and 48: arriers prevent individuals from ac
- Page 49 and 50: CHAPTERTHREEChallenges in extending
- Page 51 and 52: sources of sexual and reproductive
- Page 53 and 54: messages were delivered via a numbe
- Page 55 and 56: Ricardo, 2005). Moreover, young and
- Page 58 and 59: per cent in Guatemala. Across all c
- Page 60 and 61: tTeenager inMadagascar listens toa
- Page 62 and 63: Consensual unions account for an in
- Page 64 and 65: when. The proportion of never-marri
- Page 66 and 67: 63 per cent to 93 per cent of young
- Page 68 and 69: Family planning in humanitariansett
- Page 71 and 72: Studies suggest that HIV may have a
- Page 73: with a public health challenge (Wor
- Page 77 and 78: people in mobile, temporary, and re
- Page 79 and 80: systems and civic participation to
- Page 81 and 82: CHAPTERFOURThe social and economici
- Page 83 and 84: tCommunityeducation inCaracas, Vene
- Page 85 and 86: Estimates of Total Fertility2010-20
- Page 87 and 88: children, and healthier women also
- Page 89 and 90: empirical evidence supporting this
- Page 92 and 93: tRicardo and Sarain Mexico City say
- Page 94 and 95: to secure the future population’s
- Page 96 and 97: 86 CHAPTER 5: THE COSTS AND SAVINGS
- Page 98 and 99: Unintended Pregnancies and outcomes
- Page 100 and 101: tDonor Commitmentspanel at the Lond
- Page 102 and 103: UNFPA supports the Health for All c
- Page 104 and 105: tDr. BabatundeOsotimehin, Executive
- Page 106 and 107: 96 CHAPTER 6: MAKING THE RIGHT TO F
- Page 108 and 109: When individuals are able to exerci
- Page 110 and 111: Family planning programmes must ref
- Page 112 and 113: Family planning programmes reinforc
- Page 114: tPresident of NigeriaGoodluck Jonat
- Page 117 and 118: Monitoring Monitoring ICPD ICPD Goa
- Page 119 and 120: Monitoring Monitoring ICPD ICPD Goa
- Page 121 and 122: Monitoring Monitoring ICPD ICPD Goa
- Page 123 and 124: Monitoring ICPD Goals Demographic -
- Page 125 and 126:
Monitoring ICPD Goals - Selected In
- Page 127 and 128:
BibliographyAbbasi-Shavazi, Mohamma
- Page 129 and 130:
Monitoring ICPD Goals - Selected In
- Page 131 and 132:
Monitoring ICPD Goals - Selected In
- Page 133 and 134:
Monitoring ICPD Goals - Selected In
- Page 135 and 136:
Monitoring ICPD Goals - Selected In
- Page 137 and 138:
Monitoring ICPD Goals - Selected In
- Page 140:
Delivering a world where every preg