63 per cent to 93 per cent <strong>of</strong> young men reportingusing contraception in parts <strong>of</strong> NorthAmerica, Europe, and Latin America and theCaribbean (United Nations, 2007). These figuresstand in stark contrast with most sub-SaharanAfrican countries, where less than 50 per cent<strong>of</strong> young, sexually active men used a condom atlast sex. Globally, female sterilization remains themost commonly used method, chosen by 20 percent <strong>of</strong> married women (United Nations, 2011).The figure is much higher in some countriesdepending on fertility patterns and the range<strong>of</strong> reversible methods available to women.Countries, with the support <strong>of</strong> the international community,should protect and promote the rights <strong>of</strong> adolescents toreproductive health education, information and care andgreatly reduce the number <strong>of</strong> adolescent pregnancies …Governments, in collaboration with non-governmentalorganizations, are urged to meet the special needs <strong>of</strong>adolescents and to establish appropriate programmes torespond to those needs. Such programmes should includesupport mechanisms for the education and counseling <strong>of</strong>adolescents in the areas <strong>of</strong> gender relations and equality,violence against adolescents, responsible sexual behaviour,responsible family-planning practice, family life, reproductivehealth, sexually transmitted diseases, HIV infection andAIDS prevention.— ICPD Programme <strong>of</strong> Action, paragraphs 7.46 and 7.47.The international community has morethoroughly cultivated men’s engagement in thecontext <strong>of</strong> HIV prevention, and communitybasedprevention efforts have contributed toincreased uptake <strong>of</strong> male condoms. Yet the<strong>World</strong> Health Organization reports that lessthan a third (31 per cent) <strong>of</strong> young men indeveloping countries have a “thorough andaccurate” understanding <strong>of</strong> HIV, suggesting thatmore support for men’s sexual and reproductivehealth, including sexuality education and contraceptives,is needed (United Nations, 2009b).Men are increasingly expressing a desire tobe more engaged in planning their families,including reducing the number <strong>of</strong> unplannedpregnancies (Barker and Pawlak, 2011). Up to50 per cent <strong>of</strong> men in some countries—Brazil,Germany, Mexico, Spain, and the United<strong>State</strong>s—would consider hormone-based contraceptionif such male methods became available(Glasier, 2010). Involving men <strong>of</strong> reproductiveage in family planning programmes from anearly age can promote more constructive communicationbetween couples about the timingand spacing <strong>of</strong> children.4 Other marginalized groupsIndigenous people and ethnic minorities.Indigenous peoples and ethnic minorities <strong>of</strong>tenlack access to family planning. Results fromqualitative interviews find that providers themselvesexpress difficulties assisting ethnic andindigenous women, <strong>of</strong>ten because <strong>of</strong> an inabilityto adequately communicate or understandtheir cultural practices (Silva and Batista, 2010;Cooper, 2005). Prejudice against these groupscan lead to lower levels <strong>of</strong> investment in theirsexual and reproductive health (United NationsEconomic and Social Council, 2009).The harmful consequences <strong>of</strong> governmentunder-investment are reflected in large disparitiesbetween indigenous and non-indigenous womenon key reproductive and maternal health indicators.These include maternal mortality rates,total fertility rates and unmet need for familyplanning (Silva and Batista, 2010).Significant health-related inequalities existbetween indigenous and non-indigenousgroups in several countries around the world.In Guatemala, for example, where indigenous56 CHAPTER 3: CHALLENGES IN EXTENDING ACCESS TO EVERYONE
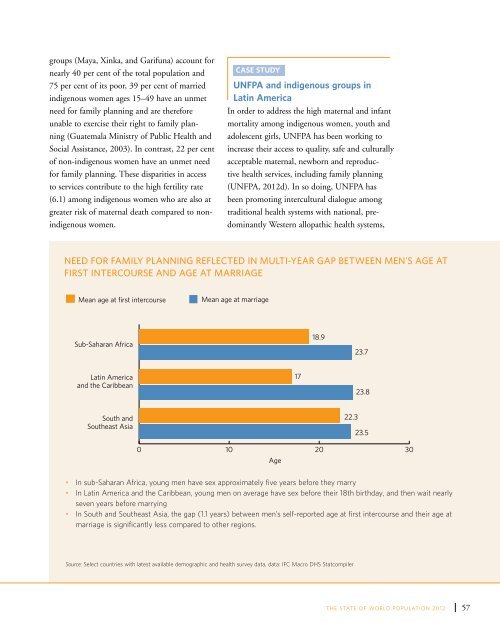
groups (Maya, Xinka, and Garifuna) account fornearly 40 per cent <strong>of</strong> the total population and75 per cent <strong>of</strong> its poor, 39 per cent <strong>of</strong> marriedindigenous women ages 15–49 have an unmetneed for family planning and are thereforeunable to exercise their right to family planning(Guatemala Ministry <strong>of</strong> Public Health andSocial Assistance, 2003). In contrast, 22 per cent<strong>of</strong> non-indigenous women have an unmet needfor family planning. These disparities in accessto services contribute to the high fertility rate(6.1) among indigenous women who are also atgreater risk <strong>of</strong> maternal death compared to nonindigenouswomen.CASE STUDY<strong>UNFPA</strong> and indigenous groups inLatin AmericaIn order to address the high maternal and infantmortality among indigenous women, youth andadolescent girls, <strong>UNFPA</strong> has been working toincrease their access to quality, safe and culturallyacceptable maternal, newborn and reproductivehealth services, including family planning(<strong>UNFPA</strong>, <strong>2012</strong>d). In so doing, <strong>UNFPA</strong> hasbeen promoting intercultural dialogue amongtraditional health systems with national, predominantlyWestern allopathic health systems,Need for family planning reflected in multi-year gap between men’s age atfirst intercourse and age at marriageMean age at first intercourseMean age at marriageSub-Saharan Africa18.923.7Latin Americaand the Caribbean1723.8South andSoutheast Asia22.323.50 10 20 30Age• In sub-Saharan Africa, young men have sex approximately five years before they marry• In Latin America and the Caribbean, young men on average have sex before their 18th birthday, and then wait nearlyseven years before marrying• In South and Southeast Asia, the gap (1.1 years) between men’s self-reported age at first intercourse and their age atmarriage is significantly less compared to other regions.Source: Select countries with latest available demographic and health survey data, data: IFC Macro DHS StatcompilerTHE STATE OF WORLD POPULATION <strong>2012</strong>57
- Page 6 and 7:
OverviewOne hundred seventy-nine go
- Page 8 and 9:
The report is structured to answer
- Page 10 and 11:
viiiCHAPTER 1: THE RIGHT TO FAMILY
- Page 12 and 13:
“All human beings are born free a
- Page 14 and 15:
Treaties, conventions and agreement
- Page 16 and 17: Health: a social and economic right
- Page 18: “Everyone has the right to educat
- Page 21 and 22: designing and delivering accessible
- Page 23 and 24: use, and reduces unintended pregnan
- Page 26 and 27: 16 CHAPTER 2: ANALYSING DATA AND TR
- Page 28 and 29: Change in Age-Specific Fertility Ra
- Page 30 and 31: Sexuality, sexual and gender stereo
- Page 32 and 33: not necessarily associated with a d
- Page 34 and 35: METHOD EFFECTIVENESSMethod, rankedf
- Page 36 and 37: tCouple visiting a ruralfamily plan
- Page 38: Demand and supply over time5 per ce
- Page 41 and 42: contribute to high unmet need (Sing
- Page 43 and 44: abortions in the region lead to mor
- Page 45 and 46: (as stated in the Convention on the
- Page 47 and 48: arriers prevent individuals from ac
- Page 49 and 50: CHAPTERTHREEChallenges in extending
- Page 51 and 52: sources of sexual and reproductive
- Page 53 and 54: messages were delivered via a numbe
- Page 55 and 56: Ricardo, 2005). Moreover, young and
- Page 58 and 59: per cent in Guatemala. Across all c
- Page 60 and 61: tTeenager inMadagascar listens toa
- Page 62 and 63: Consensual unions account for an in
- Page 64 and 65: when. The proportion of never-marri
- Page 68 and 69: Family planning in humanitariansett
- Page 71 and 72: Studies suggest that HIV may have a
- Page 73 and 74: with a public health challenge (Wor
- Page 75 and 76: State-run family planning programme
- Page 77 and 78: people in mobile, temporary, and re
- Page 79 and 80: systems and civic participation to
- Page 81 and 82: CHAPTERFOURThe social and economici
- Page 83 and 84: tCommunityeducation inCaracas, Vene
- Page 85 and 86: Estimates of Total Fertility2010-20
- Page 87 and 88: children, and healthier women also
- Page 89 and 90: empirical evidence supporting this
- Page 92 and 93: tRicardo and Sarain Mexico City say
- Page 94 and 95: to secure the future population’s
- Page 96 and 97: 86 CHAPTER 5: THE COSTS AND SAVINGS
- Page 98 and 99: Unintended Pregnancies and outcomes
- Page 100 and 101: tDonor Commitmentspanel at the Lond
- Page 102 and 103: UNFPA supports the Health for All c
- Page 104 and 105: tDr. BabatundeOsotimehin, Executive
- Page 106 and 107: 96 CHAPTER 6: MAKING THE RIGHT TO F
- Page 108 and 109: When individuals are able to exerci
- Page 110 and 111: Family planning programmes must ref
- Page 112 and 113: Family planning programmes reinforc
- Page 114: tPresident of NigeriaGoodluck Jonat
- Page 117 and 118:
Monitoring Monitoring ICPD ICPD Goa
- Page 119 and 120:
Monitoring Monitoring ICPD ICPD Goa
- Page 121 and 122:
Monitoring Monitoring ICPD ICPD Goa
- Page 123 and 124:
Monitoring ICPD Goals Demographic -
- Page 125 and 126:
Monitoring ICPD Goals - Selected In
- Page 127 and 128:
BibliographyAbbasi-Shavazi, Mohamma
- Page 129 and 130:
Monitoring ICPD Goals - Selected In
- Page 131 and 132:
Monitoring ICPD Goals - Selected In
- Page 133 and 134:
Monitoring ICPD Goals - Selected In
- Page 135 and 136:
Monitoring ICPD Goals - Selected In
- Page 137 and 138:
Monitoring ICPD Goals - Selected In
- Page 140:
Delivering a world where every preg