school or work, transport costs for medical care, loss of income, school withdrawal,psychological/emotional trauma, for the individual, his/her family, the work place, and,ultimately, for the nation’s economy. HIV/<strong>AIDS</strong> has a multi-dimensional impact on acountry affecting social, demographic, economic and structural factors, not least, thehealth sector, family welfare and households, the education sector, business enterprisesand workplaces, and manpower resources. This wide spectrum of impact has beendocumented for Africa i but less so for affected countries in Asia. The recent UnitedNations Millennium Development Goals report commended Malaysia on its recordtowards achieving all MDG targets by 2015 except in halting and reversing the spread ofHIV/<strong>AIDS</strong> (UNDP 2005). An escalation of the HIV epidemic would seriously underminethe pace of socio-economic progress and the Nation’s Vision towards developed status by2020.Profile of HIV in MalaysiaSince the disease emerged in the mid-Eighties, the profile of reported HIV infections hasremained consistent, i.e., predominantly substance abusers (IDUs), male, 20-39 years ofage, Malaysian Malay ethnicity and heterosexual (Figure 1). The relatively young agegroupaffected implicates losses in human capital investments and productive resources.Furthermore, despite the preventive measures thus far, the persistence of the substanceabuse and dependence problem in Malaysia provides a continuous human pool ofpotential HIV infections. To reduce <strong>this</strong> risk, the Ministry of Health (MOH) andMalaysian <strong>AIDS</strong> Council (MAC) initiated the Harm Reduction programme in December2005 which will be expanded under the 2006-2010 National Strategic Plan on HIV/<strong>AIDS</strong>(MOH 2006b).Despite the preponderance of infected men, there is serious concern over the risingnumbers of women infected with HIV. Women with HIV bear the added risk of verticaltransmission to infants. In addition, although the present numbers and proportion aresmall, there also appears to be a rising trend in new HIV infections classified as MSMtransmission.14
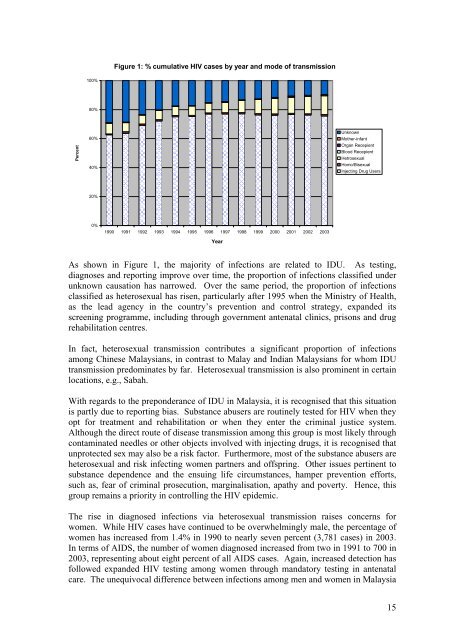
Figure 1: % cumulative HIV cases by year and mode of transmission100%80%Percent60%40%UnknownMother-infantOrgan RecepientBlood RecepientHetrosexualHomo/BisexualInjecting Drug Users20%0%1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003YearAs shown in Figure 1, the majority of infections are related to IDU. As testing,diagnoses and reporting improve over time, the proportion of infections classified underunknown causation has narrowed. Over the same period, the proportion of infectionsclassified as heterosexual has risen, particularly after 1995 when the Ministry of Health,as the lead agency in the country’s prevention and control strategy, expanded itsscreening programme, including through government antenatal clinics, prisons and drugrehabilitation centres.In fact, heterosexual transmission contributes a significant proportion of infectionsamong Chinese Malaysians, in contrast to Malay and Indian Malaysians for whom IDUtransmission predominates by far. Heterosexual transmission is also prominent in certainlocations, e.g., Sabah.With regards to the preponderance of IDU in Malaysia, it is recognised that <strong>this</strong> situationis partly due to reporting bias. Substance abusers are routinely tested for HIV when theyopt for treatment and rehabilitation or when they enter the criminal justice system.Although the direct route of disease transmission among <strong>this</strong> group is most likely throughcontaminated needles or other objects involved with injecting drugs, it is recognised thatunprotected sex may also be a risk factor. Furthermore, most of the substance abusers areheterosexual and risk infecting women partners and offspring. Other issues pertinent tosubstance dependence and the ensuing life circumstances, hamper prevention efforts,such as, fear of criminal prosecution, marginalisation, apathy and poverty. Hence, <strong>this</strong>group remains a priority in controlling the HIV epidemic.The rise in diagnosed infections via heterosexual transmission raises concerns forwomen. While HIV cases have continued to be overwhelmingly male, the percentage ofwomen has increased from 1.4% in 1990 to nearly seven percent (3,781 cases) in 2003.In terms of <strong>AIDS</strong>, the number of women diagnosed increased from two in 1991 to 700 in2003, representing about eight percent of all <strong>AIDS</strong> cases. Again, increased detection hasfollowed expanded HIV testing among women through mandatory testing in antenatalcare. The unequivocal difference between infections among men and women in Malaysia15
- Page 2 and 3: Table of ContentsPROJECT TEAM 5ACKN
- Page 4 and 5: Information received at the time of
- Page 6 and 7: AcknowledgementsThis research is fu
- Page 9: The main findings from the qualitat
- Page 16 and 17: is that the large majority of women
- Page 18 and 19: In fact, special surveys conducted
- Page 20 and 21: ObjectivesThe specific objectives o
- Page 22 and 23: have been rejected by their immedia
- Page 24 and 25: eport) that his/her healthcare (or
- Page 26 and 27: CommunityKnowledge/awareness of HIV
- Page 28 and 29: Framework of analysisA descriptive
- Page 30 and 31: urban and a rural community. In all
- Page 32 and 33: medication, the physical health com
- Page 34 and 35: husbands working in other places wh
- Page 36 and 37: (“And then, this doctor, he/she v
- Page 38 and 39: their food. Nurses and their attend
- Page 40 and 41: “Because we take drugs….no time
- Page 42 and 43: The same claim to 100% condom use w
- Page 44 and 45: in asking them to use condoms, even
- Page 46 and 47: “Normally…..normally, memang ma
- Page 48 and 49: (“But I continued using at that t
- Page 50 and 51: “Buat pada permulaannya, saya mem
- Page 52 and 53: However, not all experiences with d
- Page 54 and 55: yang amat sangat. Tak pernah I rasa
- Page 56 and 57: long term fears and anxieties. The
- Page 58 and 59: “The first time I heard from the
- Page 60 and 61: handset, I too, have handset. Some
- Page 62 and 63: have been turning to God since and
- Page 64 and 65:
felt I’m indecent. But, at one ti
- Page 66 and 67:
would certainly want to continue wo
- Page 68 and 69:
(Transgender, 53 yrs, Upper seconda
- Page 70 and 71:
“Sometimes I didn’t get enough
- Page 72 and 73:
positively portray people living wi
- Page 74 and 75:
“After my diagnosis...I’ll pay
- Page 76 and 77:
not know or might not want to be bo
- Page 78 and 79:
(UNAIDS 2005).(UNAIDS 2000):The fac
- Page 80 and 81:
“…bawak saya pergi hospital. An
- Page 82 and 83:
erpindah ke tempat lain makin lama.
- Page 84 and 85:
pada HIV itu, dia nampak penagih. S
- Page 86 and 87:
(Male, 49yrs, University education,
- Page 88 and 89:
However this association with the n
- Page 90 and 91:
“…..depends on who is the perso
- Page 92 and 93:
(“I …my experience society will
- Page 94 and 95:
(“Can…can marry, no problem. Bu
- Page 96 and 97:
Harm Reduction programmeSome urban
- Page 98 and 99:
(“In my opinion such campaign sta
- Page 100 and 101:
Table 2aDistribution of Respondents
- Page 102 and 103:
female sex workers (seven out of 13
- Page 104 and 105:
NO. OF LIVING PARENTSNobody 7 1 1 2
- Page 106 and 107:
tested in drug rehabilitation cente
- Page 108 and 109:
GroupsDUHetero-SexuallyInfectedMenT
- Page 110 and 111:
y the Ministry of Health (74.2%) or
- Page 113 and 114:
Child CareYes, often 0 0 0 1 0 1 0
- Page 115 and 116:
GroupsDUHetero-SexuallyInfectedMenT
- Page 117 and 118:
Figure 5: Percentage of Respondents
- Page 119 and 120:
GroupsTable 12aEmotional Problems E
- Page 121 and 122:
Stigmatization and how it has affec
- Page 123 and 124:
GroupsTable 15How They Cope With Th
- Page 125 and 126:
Table 18Percentage Of Respondents W
- Page 127 and 128:
esponsible for their families. As m
- Page 129 and 130:
In this study, it took more effort
- Page 131 and 132:
eing transgender and sex worker whe
- Page 133 and 134:
denies them social and economic opp
- Page 135 and 136:
working towards their future, who c
- Page 137 and 138:
ReferencesAidsmeds.com (2006). Curr
- Page 139 and 140:
Sen G, George A, Ostlin P (2002). E
- Page 141 and 142:
Annex II: FGD Guide for PLHIV Group
- Page 143 and 144:
♦ Spouse: marital/sexual relation
- Page 145 and 146:
I. Attitudes and Perceptions relate
- Page 147 and 148:
I. HIV/AIDS Knowledge‣ What did y
- Page 149 and 150:
Annex V: Rapid Needs Assessment Que
- Page 151 and 152:
Types of support or responsibilityM
- Page 153 and 154:
Please tick (√)one onlyIf yes,ple
- Page 155 and 156:
more help would be useful for you i
- Page 157 and 158:
Annex VI: Ethics Approval Letter157