(“In my opinion such campaign starts from the home”)(Rural, Malay, Male)“If children means parents should take care”(Urban, Indian, Female)“Sex education memang perlu…sekolah menengah. Sebab pelajar-pelajarini terlalu terpengaruh ..apa…they attracted to outside world. So. Jadi sexeducation, drug education mesti nak beri”(“Sex education is needed…secondary school. Because students are vermuch influenced…they are attracted to the outside world…So sexeducation, drug education must be given”)(Urban, Indian, Female)National Service was also mentioned as an opportunity to impart knowledge of HIV toyoung people. Factory workers and foreign workers were two other populations whichparticipants felt that we could target.In terms of approach participants suggested:• Awareness campaigns on a wide scale so that it can also reach the rural areas• Control of the internet• Testing of Tourists• Education for foreign workers both legal as well as the illegalIn summary, twenty years into the epidemic yet the knowledge of community is shallow.The community has heard of the terms “HIV’ and “<strong>AIDS</strong>” but the details of transmissionare not clearly known. Only once in the four FGDs on community was there mention of“unprotected sex” as the cause. It was always moral loaded terms “free sex”, sex outsideof marriage that cause the spread. The blame on drugs is universal partly because of themedia and the manner we collect data in the country. Stigma, which is rampant in ourcommunity, is not really perceived as such by participants. Participants expressstatements such as “We must show sympathy”, “…support”, etc., “like all goodneighbours but we must be cautious”, “…cautious with our children playing with them”,“….with the food they offer us in return” (as most good neighbours do).For those aware of the process, <strong>this</strong> fear of infection is reinforced by the manner in whichthe remains of <strong>AIDS</strong> infected relatives is prepared for burial. The stigma from societythat PLHIVs often perceive and express is, in fact, supported by reality. Clearly, thegeneral community has yet to internalize the messages that HIV cannot be transmittedthrough touch or food. Furthermore, there are many who do not realise that by sayingthat they need to exercise caution when mixing with a certain group they are, in fact,manifesting stigma and discrimination. Possibly, the HIV epidemic has to reach theproportion of drug abuse in <strong>this</strong> country, i.e., when having an infected family memberbecomes so common-place, before society starts to believe that it cannot spread throughthose means.98
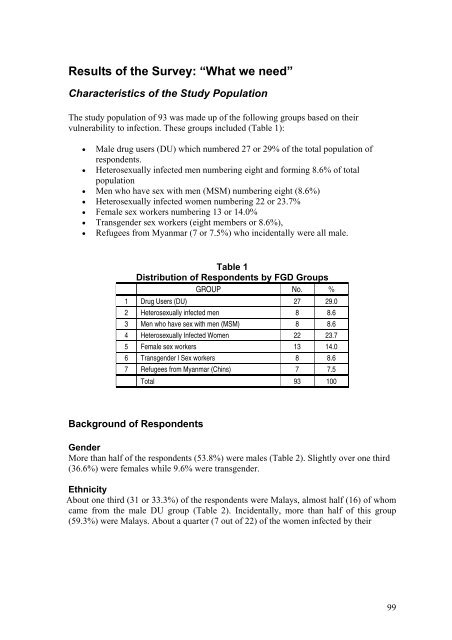
Results of the Survey: “What we need”Characteristics of the Study PopulationThe study population of 93 was made up of the following groups based on theirvulnerability to infection. These groups included (Table 1):• Male drug users (DU) which numbered 27 or 29% of the total population ofrespondents.• Heterosexually infected men numbering eight and forming 8.6% of totalpopulation• Men who have sex with men (MSM) numbering eight (8.6%)• Heterosexually infected women numbering 22 or 23.7%• Female sex workers numbering 13 or 14.0%• Transgender sex workers (eight members or 8.6%),• Refugees from Myanmar (7 or 7.5%) who incidentally were all male.Table 1Distribution of Respondents by FGD GroupsGROUP No. %1 Drug Users (DU) 27 29.02 Heterosexually infected men 8 8.63 Men who have sex with men (MSM) 8 8.64 Heterosexually Infected Women 22 23.75 Female sex workers 13 14.06 Transgender l Sex workers 8 8.67 Refugees from Myanmar (Chins) 7 7.5Total 93 100Background of RespondentsGenderMore than half of the respondents (53.8%) were males (Table 2). Slightly over one third(36.6%) were females while 9.6% were transgender.EthnicityAbout one third (31 or 33.3%) of the respondents were Malays, almost half (16) of whomcame from the male DU group (Table 2). Incidentally, more than half of <strong>this</strong> group(59.3%) were Malays. About a quarter (7 out of 22) of the women infected by their99
- Page 2 and 3:
Table of ContentsPROJECT TEAM 5ACKN
- Page 4 and 5:
Information received at the time of
- Page 6 and 7:
AcknowledgementsThis research is fu
- Page 9:
The main findings from the qualitat
- Page 14 and 15:
school or work, transport costs for
- Page 16 and 17:
is that the large majority of women
- Page 18 and 19:
In fact, special surveys conducted
- Page 20 and 21:
ObjectivesThe specific objectives o
- Page 22 and 23:
have been rejected by their immedia
- Page 24 and 25:
eport) that his/her healthcare (or
- Page 26 and 27:
CommunityKnowledge/awareness of HIV
- Page 28 and 29:
Framework of analysisA descriptive
- Page 30 and 31:
urban and a rural community. In all
- Page 32 and 33:
medication, the physical health com
- Page 34 and 35:
husbands working in other places wh
- Page 36 and 37:
(“And then, this doctor, he/she v
- Page 38 and 39:
their food. Nurses and their attend
- Page 40 and 41:
“Because we take drugs….no time
- Page 42 and 43:
The same claim to 100% condom use w
- Page 44 and 45:
in asking them to use condoms, even
- Page 46 and 47:
“Normally…..normally, memang ma
- Page 48 and 49: (“But I continued using at that t
- Page 50 and 51: “Buat pada permulaannya, saya mem
- Page 52 and 53: However, not all experiences with d
- Page 54 and 55: yang amat sangat. Tak pernah I rasa
- Page 56 and 57: long term fears and anxieties. The
- Page 58 and 59: “The first time I heard from the
- Page 60 and 61: handset, I too, have handset. Some
- Page 62 and 63: have been turning to God since and
- Page 64 and 65: felt I’m indecent. But, at one ti
- Page 66 and 67: would certainly want to continue wo
- Page 68 and 69: (Transgender, 53 yrs, Upper seconda
- Page 70 and 71: “Sometimes I didn’t get enough
- Page 72 and 73: positively portray people living wi
- Page 74 and 75: “After my diagnosis...I’ll pay
- Page 76 and 77: not know or might not want to be bo
- Page 78 and 79: (UNAIDS 2005).(UNAIDS 2000):The fac
- Page 80 and 81: “…bawak saya pergi hospital. An
- Page 82 and 83: erpindah ke tempat lain makin lama.
- Page 84 and 85: pada HIV itu, dia nampak penagih. S
- Page 86 and 87: (Male, 49yrs, University education,
- Page 88 and 89: However this association with the n
- Page 90 and 91: “…..depends on who is the perso
- Page 92 and 93: (“I …my experience society will
- Page 94 and 95: (“Can…can marry, no problem. Bu
- Page 96 and 97: Harm Reduction programmeSome urban
- Page 100 and 101: Table 2aDistribution of Respondents
- Page 102 and 103: female sex workers (seven out of 13
- Page 104 and 105: NO. OF LIVING PARENTSNobody 7 1 1 2
- Page 106 and 107: tested in drug rehabilitation cente
- Page 108 and 109: GroupsDUHetero-SexuallyInfectedMenT
- Page 110 and 111: y the Ministry of Health (74.2%) or
- Page 113 and 114: Child CareYes, often 0 0 0 1 0 1 0
- Page 115 and 116: GroupsDUHetero-SexuallyInfectedMenT
- Page 117 and 118: Figure 5: Percentage of Respondents
- Page 119 and 120: GroupsTable 12aEmotional Problems E
- Page 121 and 122: Stigmatization and how it has affec
- Page 123 and 124: GroupsTable 15How They Cope With Th
- Page 125 and 126: Table 18Percentage Of Respondents W
- Page 127 and 128: esponsible for their families. As m
- Page 129 and 130: In this study, it took more effort
- Page 131 and 132: eing transgender and sex worker whe
- Page 133 and 134: denies them social and economic opp
- Page 135 and 136: working towards their future, who c
- Page 137 and 138: ReferencesAidsmeds.com (2006). Curr
- Page 139 and 140: Sen G, George A, Ostlin P (2002). E
- Page 141 and 142: Annex II: FGD Guide for PLHIV Group
- Page 143 and 144: ♦ Spouse: marital/sexual relation
- Page 145 and 146: I. Attitudes and Perceptions relate
- Page 147 and 148: I. HIV/AIDS Knowledge‣ What did y
- Page 149 and 150:
Annex V: Rapid Needs Assessment Que
- Page 151 and 152:
Types of support or responsibilityM
- Page 153 and 154:
Please tick (√)one onlyIf yes,ple
- Page 155 and 156:
more help would be useful for you i
- Page 157 and 158:
Annex VI: Ethics Approval Letter157