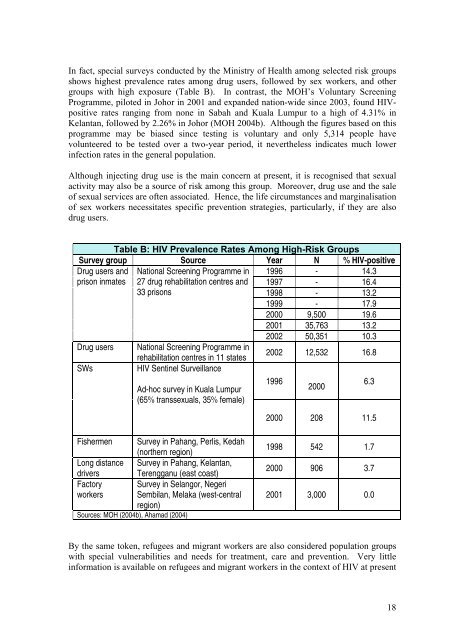
In fact, special surveys conducted by the Ministry of Health among selected risk groupsshows highest prevalence rates among drug users, followed by sex workers, and othergroups with high exposure (Table B). In contrast, the MOH’s Voluntary ScreeningProgramme, piloted in Johor in 2001 and expanded nation-wide since 2003, found HIVpositiverates ranging from none in Sabah and Kuala Lumpur to a high of 4.31% inKelantan, followed by 2.26% in Johor (MOH 2004b). Although the figures based on <strong>this</strong>programme may be biased since testing is voluntary and only 5,314 people havevolunteered to be tested over a two-year period, it nevertheless indicates much lowerinfection rates in the general population.Although injecting drug use is the main concern at present, it is recognised that sexualactivity may also be a source of risk among <strong>this</strong> group. Moreover, drug use and the saleof sexual services are often associated. Hence, the life circumstances and marginalisationof sex workers necessitates specific prevention strategies, particularly, if they are alsodrug users.Table B: HIV Prevalence Rates Among High-Risk GroupsSurvey group Source Year N % HIV-positiveDrug users and National Screening Programme in 1996 - 14.3prison inmates 27 drug rehabilitation centres and 1997 - 16.433 prisons1998 - 13.21999 - 17.92000 9,500 19.62001 35,763 13.22002 50,351 10.3Drug users National Screening Programme inrehabilitation centres in 11 states2002 12,532 16.8SWsHIV Sentinel SurveillanceAd-hoc survey in Kuala Lumpur(65% transsexuals, 35% female)199620006.32000 208 11.5Fishermen Survey in Pahang, Perlis, Kedah(northern region)Long distance Survey in Pahang, Kelantan,drivers Terengganu (east coast)Factory Survey in Selangor, Negeriworkers Sembilan, Melaka (west-centralregion)Sources: MOH (2004b), Ahamad (2004)1998 542 1.72000 906 3.72001 3,000 0.0By the same token, refugees and migrant workers are also considered population groupswith special vulnerabilities and needs for treatment, care and prevention. Very littleinformation is available on refugees and migrant workers in the context of HIV at present18
although there are millions in Malaysia, a significant proportion of whom remainundocumented.Rationale for projectThere has been no published study on the impact of HIV/<strong>AIDS</strong> in Malaysia. The impactof HIV/<strong>AIDS</strong> manifests at both micro- and macro-levels. At the micro-level, impactincludes the social, psychological, health and economic consequences for PLHIV andtheir families/care-givers. At the macro-level, HIV/<strong>AIDS</strong> can be positioned within adevelopment context that has potential impact on various sectors, such as Education,Healthcare, Social Welfare, Population/Demography, Labour, Industry and BusinessEnterprise.At the micro-level, the personal experiences of PLHIV related to their HIV and <strong>AIDS</strong>have been reported (e.g., Sam 2002; Zaiton 2002; MAC 1999). However, although theseprovide interesting and useful narratives, they have not focussed on the impact of thedisease in a framework with policy considerations. The present study proposes aqualitative approach to systematically document and analyse the impact of the disease oninfected and affected people’s lives from various perspectives based on the differentbackgrounds of HIV transmission. In particular, the study will document theconsequences of being HIV-infected in the context of individual, family and societalfactors, including public policy.Furthermore, a recent consultative report on obstacles in scaling-up the national responseto HIV/<strong>AIDS</strong> identified, among others, continued stigmatization and discrimination, lowparticipation of PLHIV in planning, implementing and utilising prevention and treatmentprogrammes, and poor programme monitoring and evaluation (MOH 2006c). A study todocument the various dimensions of the impact of HIV/<strong>AIDS</strong> on the personal lives and ofaffected families will provide the baseline information to strengthen and enhancestrategies in the national response to HIV/<strong>AIDS</strong>. Similarly, a monitoring and evaluation(M&E) system is predicated on rational programme planning, which in turn, should bebased on assessment of needs.Within the rationale of <strong>this</strong> project are the underlying principles of: greater involvement of PLHIVs (GIPA) – to assess information from the targetpopulation in order to frame policies that can better address their needs; the growing feminization of the epidemic – to better understand the specificvulnerability of women to HIV and how they are infected from their partners andenable a gender-focussed perspective to the debates on HIV in Malaysia; Increasing access to HIV prevention, treatment, care and support – to comprehend therealities and barriers in the lives of PLHIV community and how policies affect them; the Three Ones approach - One comprehensive HIV/<strong>AIDS</strong> framework; One nationalHIV/<strong>AIDS</strong> authority with broad multisectoral support; One monitoring andevaluation (M&E) system integrated into the <strong>AIDS</strong> framework with a set ofstandardised indicators - by strengthening the information base towards a greaterunderstanding of the processes and consequences of HIV/<strong>AIDS</strong>, beyond merenumbers.19
- Page 2 and 3: Table of ContentsPROJECT TEAM 5ACKN
- Page 4 and 5: Information received at the time of
- Page 6 and 7: AcknowledgementsThis research is fu
- Page 9: The main findings from the qualitat
- Page 14 and 15: school or work, transport costs for
- Page 16 and 17: is that the large majority of women
- Page 20 and 21: ObjectivesThe specific objectives o
- Page 22 and 23: have been rejected by their immedia
- Page 24 and 25: eport) that his/her healthcare (or
- Page 26 and 27: CommunityKnowledge/awareness of HIV
- Page 28 and 29: Framework of analysisA descriptive
- Page 30 and 31: urban and a rural community. In all
- Page 32 and 33: medication, the physical health com
- Page 34 and 35: husbands working in other places wh
- Page 36 and 37: (“And then, this doctor, he/she v
- Page 38 and 39: their food. Nurses and their attend
- Page 40 and 41: “Because we take drugs….no time
- Page 42 and 43: The same claim to 100% condom use w
- Page 44 and 45: in asking them to use condoms, even
- Page 46 and 47: “Normally…..normally, memang ma
- Page 48 and 49: (“But I continued using at that t
- Page 50 and 51: “Buat pada permulaannya, saya mem
- Page 52 and 53: However, not all experiences with d
- Page 54 and 55: yang amat sangat. Tak pernah I rasa
- Page 56 and 57: long term fears and anxieties. The
- Page 58 and 59: “The first time I heard from the
- Page 60 and 61: handset, I too, have handset. Some
- Page 62 and 63: have been turning to God since and
- Page 64 and 65: felt I’m indecent. But, at one ti
- Page 66 and 67: would certainly want to continue wo
- Page 68 and 69:
(Transgender, 53 yrs, Upper seconda
- Page 70 and 71:
“Sometimes I didn’t get enough
- Page 72 and 73:
positively portray people living wi
- Page 74 and 75:
“After my diagnosis...I’ll pay
- Page 76 and 77:
not know or might not want to be bo
- Page 78 and 79:
(UNAIDS 2005).(UNAIDS 2000):The fac
- Page 80 and 81:
“…bawak saya pergi hospital. An
- Page 82 and 83:
erpindah ke tempat lain makin lama.
- Page 84 and 85:
pada HIV itu, dia nampak penagih. S
- Page 86 and 87:
(Male, 49yrs, University education,
- Page 88 and 89:
However this association with the n
- Page 90 and 91:
“…..depends on who is the perso
- Page 92 and 93:
(“I …my experience society will
- Page 94 and 95:
(“Can…can marry, no problem. Bu
- Page 96 and 97:
Harm Reduction programmeSome urban
- Page 98 and 99:
(“In my opinion such campaign sta
- Page 100 and 101:
Table 2aDistribution of Respondents
- Page 102 and 103:
female sex workers (seven out of 13
- Page 104 and 105:
NO. OF LIVING PARENTSNobody 7 1 1 2
- Page 106 and 107:
tested in drug rehabilitation cente
- Page 108 and 109:
GroupsDUHetero-SexuallyInfectedMenT
- Page 110 and 111:
y the Ministry of Health (74.2%) or
- Page 113 and 114:
Child CareYes, often 0 0 0 1 0 1 0
- Page 115 and 116:
GroupsDUHetero-SexuallyInfectedMenT
- Page 117 and 118:
Figure 5: Percentage of Respondents
- Page 119 and 120:
GroupsTable 12aEmotional Problems E
- Page 121 and 122:
Stigmatization and how it has affec
- Page 123 and 124:
GroupsTable 15How They Cope With Th
- Page 125 and 126:
Table 18Percentage Of Respondents W
- Page 127 and 128:
esponsible for their families. As m
- Page 129 and 130:
In this study, it took more effort
- Page 131 and 132:
eing transgender and sex worker whe
- Page 133 and 134:
denies them social and economic opp
- Page 135 and 136:
working towards their future, who c
- Page 137 and 138:
ReferencesAidsmeds.com (2006). Curr
- Page 139 and 140:
Sen G, George A, Ostlin P (2002). E
- Page 141 and 142:
Annex II: FGD Guide for PLHIV Group
- Page 143 and 144:
♦ Spouse: marital/sexual relation
- Page 145 and 146:
I. Attitudes and Perceptions relate
- Page 147 and 148:
I. HIV/AIDS Knowledge‣ What did y
- Page 149 and 150:
Annex V: Rapid Needs Assessment Que
- Page 151 and 152:
Types of support or responsibilityM
- Page 153 and 154:
Please tick (√)one onlyIf yes,ple
- Page 155 and 156:
more help would be useful for you i
- Page 157 and 158:
Annex VI: Ethics Approval Letter157