


You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
28 Picard, Silvy, and Gabert<br />
However, like all PCR, inaccurate results may occur because of either falsepositives<br />
due to contamination, or false-negatives as a result of (1) poor RNA<br />
quality, (2) failure of the RT and PCR steps, or (3) inappropriate primers.<br />
In acute myeloid leukemia (AML), molecular diagnosis for the optimal management<br />
of patients and for minimal residual disease (MRD) monitoring is of extreme<br />
importance. In the mid-1990s, competitive RT-PCR was successfully applied<br />
to quantify the level of fusion gene transcripts in CML and AML with either t(8;21)<br />
or inv(16). Based on the results of this method, the risk of relapse among patients<br />
with AML1-ETO and CBFB-MYH11 transcripts detected in clinical remission is<br />
correlated with the relative level of residual disease, and the kinetic of achievement<br />
of molecular remission is an independent prognostic factor (1,2). However, competitive<br />
RT-PCR is end-point PCR, requires many controls, lacks reproducibility,<br />
and necessitates labor-intensive and time-consuming practices, which prohibit both<br />
standardization and large-scale multicenter analysis.<br />
Real-time quantitative PCR (RQ-PCR) is by far the most sensitive assay in<br />
the context of MRD detection. It can detect a single leukemia cell in a background<br />
of 10 5 –10 6 normal cells. Therefore, it is quantitative to seven orders of<br />
magnitude and is up to five orders of magnitude more sensitive than other conventional<br />
methods. The inter-assay and intra-assay sensitivity of RQ-PCR is<br />
controlled by quantification of housekeeping genes. Some laboratories have<br />
demonstrated the reliability of this technology and its potential clinical value<br />
for MRD studies using fusion gene (FG) transcripts.<br />
The detection of fusion transcripts (PML-RARA, AML1–ETO, and CBFB-<br />
MYH11) by RQ-PCR both at diagnosis and for MRD analysis plays an increasing<br />
role in the management of AML patients and is prospectively being<br />
incorporated into many clinical trials. However, the real predictive clinical<br />
value of MRD detection remains to be confirmed.<br />
After an overview of the principles of RQ-PCR encompassing the chemistry,<br />
the instruments, and the primer and probe design, we will focus on more<br />
practical considerations “at the bench” and finish this overview with comments<br />
on RQ-PCR results (their expression and their interpretation).<br />
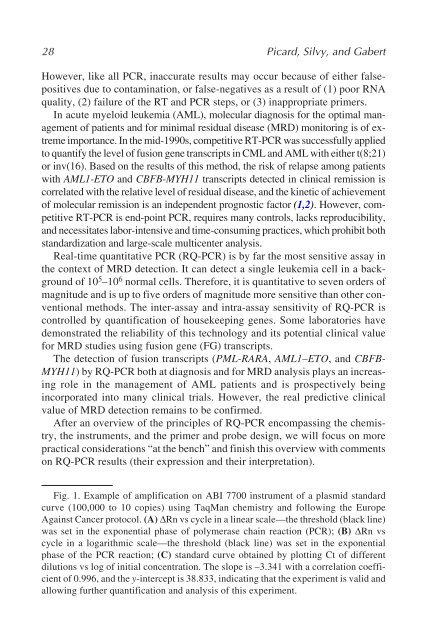
Fig. 1. Example of amplification on ABI 7700 instrument of a plasmid standard<br />
curve (100,000 to 10 copies) using TaqMan chemistry and following the Europe<br />
Against Cancer protocol. (A) ∆Rn vs cycle in a linear scale—the threshold (black line)<br />
was set in the exponential phase of polymerase chain reaction (PCR); (B) ∆Rn vs<br />
cycle in a logarithmic scale—the threshold (black line) was set in the exponential<br />
phase of the PCR reaction; (C) standard curve obtained by plotting Ct of different<br />
dilutions vs log of initial concentration. The slope is –3.341 with a correlation coefficient<br />
of 0.996, and the y-intercept is 38.833, indicating that the experiment is valid and<br />
allowing further quantification and analysis of this experiment.














