Speculum - University of Melbourne
Speculum - University of Melbourne
Speculum - University of Melbourne

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
SPECULUM 15<br />
E.C.G. DIAGNOSIS OF CONGENITAL<br />
HEART DISEASE<br />
Dr. E. R. Trethewie M.D., D.Sc., M.B., M.R.A.C.P.<br />
Reader in Physiology, <strong>University</strong> <strong>of</strong> <strong>Melbourne</strong><br />
The lesion in congenital heart disease is<br />
frequently able to be diagnosed by considering<br />
the stethoscopic and electrocardiographic<br />
findings alone. In many instances a bruit is<br />
heard in the vicinity <strong>of</strong> the second left interspace<br />
close to the sternum and it may be<br />
heard over a wide area. The bruit <strong>of</strong> pulmonary<br />
stenosis is harsh, superficial, and<br />
occupies a considerable period <strong>of</strong> systole<br />
(fig. 1). The bruit <strong>of</strong> interatrial defect has<br />
a rumbling crescendo quality with rapid<br />
diminuendo and occupies the early stage <strong>of</strong><br />
systole (fig. 4). The bruit <strong>of</strong> interventricular<br />
defect may be harsh or s<strong>of</strong>t and is<br />
frequently best heard in the fourth left interspace<br />
close to the sternum. The classical<br />
bruit <strong>of</strong> patent ductus can never be mistaken;<br />
it is a continuous machine-hum murmur;<br />
but <strong>of</strong> course, it may not produce this<br />
classical sound. It may even only be<br />
systolic in time and sometimes we think we<br />
are listening to an atypical patent ductus<br />
murmur when in reality we hear the bruit <strong>of</strong><br />
aorto-pulmonary communication.<br />
Having decided we have heard a basal<br />
bruit, usually in a young person, <strong>of</strong>ten, btit<br />
not necessarily, <strong>of</strong> inferior physique and one<br />
who has never had rheumatic fever, an examination<br />
<strong>of</strong> the electrocardiogram is<br />
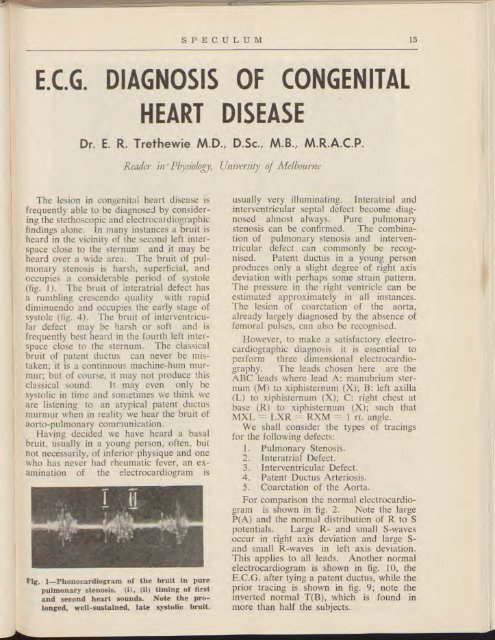
Pig. 1—Phonocardiogram <strong>of</strong> the bruit in pure<br />
pulmonary stenosis. (i), (ii) timing <strong>of</strong> first<br />
and second heart sounds. Note the prolonged,<br />
well-sustained, late systolic bruit.<br />
usually very illuminating. Interatrial and<br />
interventricular septal defect become diagnosed<br />
almost always. Pure pulmonary<br />
stenosis can be confirmed. The combination<br />
<strong>of</strong> pulmonary stenosis and interventricular<br />
defect can commonly be recognised.<br />
Patent ductus in a young person<br />
produces only a slight degree <strong>of</strong> right axis<br />
deviation with perhaps some strain pattern.<br />
The pressure in the right ventricle can be<br />
estimated approximately in all instances.<br />
The lesion <strong>of</strong> coarctation <strong>of</strong> the aorta,<br />
already largely diagnosed by the absence <strong>of</strong><br />
femoral pulses, can also be recognised.<br />
However, to make a satisfactory electrocardiographic<br />
diagnosis it is essential to<br />
perform three dimensional electrocardiography.<br />
The leads chosen here are the<br />
ABC leads where lead A: manubrium sternum<br />
(M) to xiphisternum (X); B: left axilla<br />
(L) to xiphisternum (X); C: right chest at<br />
base (R) to xiphisternum (X); such that<br />
MXL = LXR = RXM = 1 rt. angle.<br />
We shall consider the types <strong>of</strong> tracings<br />
for the following defects:<br />
1. Pulmonary Stenosis.<br />
2. Interatrial Defect.<br />
3. Interventricular Defect.<br />
4. Patent Ductus Arteriosis.<br />
5. Coarctation <strong>of</strong> the Aorta.<br />
For comparison the normal electrocardiogram<br />
is shown in fig. 2. Note the large<br />
P(A) and the normal distribution <strong>of</strong> R to S<br />
potentials. Large R- and small S-waves<br />
occur in right axis deviation and large S-<br />
and small R-waves in left axis deviation.<br />
This applies to all leads. Another normal<br />
electrocardiogram is shown in fig. 10, the<br />
E.C.G. after tying a patent ductus, while the<br />
prior tracing is shown in fig. 9; note the<br />
inverted normal T(B), which is found in<br />
more than half the subjects.