

Clinical Manual for Management of the HIV-Infected ... - myCME.com
Clinical Manual for Management of the HIV-Infected ... - myCME.com
Clinical Manual for Management of the HIV-Infected ... - myCME.com

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
3–30 | <strong>Clinical</strong> <strong>Manual</strong> <strong>for</strong> <strong>Management</strong> <strong>of</strong> <strong>the</strong> <strong>HIV</strong>-<strong>Infected</strong> Adult/2006<br />
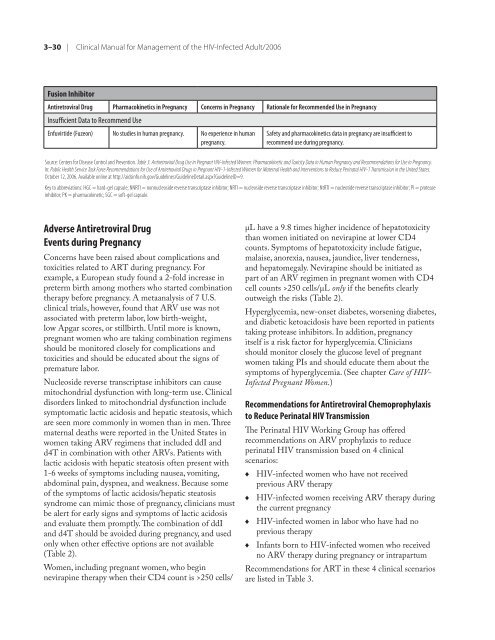
Fusion Inhibitor<br />
Antiretroviral Drug Pharmacokinetics in Pregnancy Concerns in Pregnancy Rationale <strong>for</strong> Re<strong>com</strong>mended Use in Pregnancy<br />
Insufficient Data to Re<strong>com</strong>mend Use<br />
Enfuvirtide (Fuzeon) No studies in human pregnancy. No experience in human<br />
pregnancy.<br />
Safety and pharmacokinetics data in pregnancy are insufficient to<br />
re<strong>com</strong>mend use during pregnancy.<br />
Source: Centers <strong>for</strong> Disease Control and Prevention. Table 3. Antiretroviral Drug Use in Pregnant <strong>HIV</strong>-<strong>Infected</strong> Women: Pharmacokinetic and Toxicity Data in Human Pregnancy and Re<strong>com</strong>mendations <strong>for</strong> Use in Pregnancy.<br />
In: Public Health Service Task Force Re<strong>com</strong>mendations <strong>for</strong> Use <strong>of</strong> Antiretroviral Drugs in Pregnant <strong>HIV</strong>-1-<strong>Infected</strong> Women <strong>for</strong> Maternal Health and Interventions to Reduce Perinatal <strong>HIV</strong>-1 Transmission in <strong>the</strong> United States.<br />
October 12, 2006. Available online at http://aidsinfo.nih.gov/Guidelines/GuidelineDetail.aspx?GuidelineID=9.<br />
Key to abbreviations: HGC = hard-gel capsule; NNRTI = nonnucleoside reverse transcriptase inhibitor; NRTI = nucleoside reverse transcriptase inhibitor; NtRTI = nucleotide reverse transcriptase inhibitor; PI = protease<br />
inhibitor; PK = pharmacokinetic; SGC = s<strong>of</strong>t-gel capsule.<br />
Adverse Antiretroviral Drug<br />
Events during Pregnancy<br />
Concerns have been raised about <strong>com</strong>plications and<br />
toxicities related to ART during pregnancy. For<br />
example, a European study found a 2-fold increase in<br />
preterm birth among mo<strong>the</strong>rs who started <strong>com</strong>bination<br />
<strong>the</strong>rapy be<strong>for</strong>e pregnancy. A metaanalysis <strong>of</strong> 7 U.S.<br />
clinical trials, however, found that ARV use was not<br />
associated with preterm labor, low birth-weight,<br />
low Apgar scores, or stillbirth. Until more is known,<br />
pregnant women who are taking <strong>com</strong>bination regimens<br />
should be monitored closely <strong>for</strong> <strong>com</strong>plications and<br />
toxicities and should be educated about <strong>the</strong> signs <strong>of</strong><br />
premature labor.<br />
Nucleoside reverse transcriptase inhibitors can cause<br />
mitochondrial dysfunction with long-term use. <strong>Clinical</strong><br />
disorders linked to mitochondrial dysfunction include<br />
symptomatic lactic acidosis and hepatic steatosis, which<br />
are seen more <strong>com</strong>monly in women than in men. Three<br />
maternal deaths were reported in <strong>the</strong> United States in<br />
women taking ARV regimens that included ddI and<br />
d4T in <strong>com</strong>bination with o<strong>the</strong>r ARVs. Patients with<br />
lactic acidosis with hepatic steatosis <strong>of</strong>ten present with<br />
1-6 weeks <strong>of</strong> symptoms including nausea, vomiting,<br />
abdominal pain, dyspnea, and weakness. Because some<br />
<strong>of</strong> <strong>the</strong> symptoms <strong>of</strong> lactic acidosis/hepatic steatosis<br />
syndrome can mimic those <strong>of</strong> pregnancy, clinicians must<br />
be alert <strong>for</strong> early signs and symptoms <strong>of</strong> lactic acidosis<br />
and evaluate <strong>the</strong>m promptly. The <strong>com</strong>bination <strong>of</strong> ddI<br />
and d4T should be avoided during pregnancy, and used<br />
only when o<strong>the</strong>r effective options are not available<br />
(Table 2).<br />
Women, including pregnant women, who begin<br />
nevirapine <strong>the</strong>rapy when <strong>the</strong>ir CD4 count is >250 cells/<br />
µL have a 9.8 times higher incidence <strong>of</strong> hepatotoxicity<br />
than women initiated on nevirapine at lower CD4<br />
counts. Symptoms <strong>of</strong> hepatotoxicity include fatigue,<br />
malaise, anorexia, nausea, jaundice, liver tenderness,<br />
and hepatomegaly. Nevirapine should be initiated as<br />
part <strong>of</strong> an ARV regimen in pregnant women with CD4<br />
cell counts >250 cells/µL only if <strong>the</strong> benefits clearly<br />
outweigh <strong>the</strong> risks (Table 2).<br />
Hyperglycemia, new-onset diabetes, worsening diabetes,<br />
and diabetic ketoacidosis have been reported in patients<br />
taking protease inhibitors. In addition, pregnancy<br />
itself is a risk factor <strong>for</strong> hyperglycemia. Clinicians<br />
should monitor closely <strong>the</strong> glucose level <strong>of</strong> pregnant<br />
women taking PIs and should educate <strong>the</strong>m about <strong>the</strong><br />
symptoms <strong>of</strong> hyperglycemia. (See chapter Care <strong>of</strong> <strong>HIV</strong>-<br />
<strong>Infected</strong> Pregnant Women.)<br />
Re<strong>com</strong>mendations <strong>for</strong> Antiretroviral Chemoprophylaxis<br />
to Reduce Perinatal <strong>HIV</strong> Transmission<br />
The Perinatal <strong>HIV</strong> Working Group has <strong>of</strong>fered<br />
re<strong>com</strong>mendations on ARV prophylaxis to reduce<br />
perinatal <strong>HIV</strong> transmission based on 4 clinical<br />
scenarios:<br />
♦<br />
♦<br />
♦<br />
♦<br />
<strong>HIV</strong>-infected women who have not received<br />
previous ARV <strong>the</strong>rapy<br />
<strong>HIV</strong>-infected women receiving ARV <strong>the</strong>rapy during<br />
<strong>the</strong> current pregnancy<br />
<strong>HIV</strong>-infected women in labor who have had no<br />
previous <strong>the</strong>rapy<br />
Infants born to <strong>HIV</strong>-infected women who received<br />
no ARV <strong>the</strong>rapy during pregnancy or intrapartum<br />
Re<strong>com</strong>mendations <strong>for</strong> ART in <strong>the</strong>se 4 clinical scenarios<br />
are listed in Table 3.














