

Clinical Manual for Management of the HIV-Infected ... - myCME.com
Clinical Manual for Management of the HIV-Infected ... - myCME.com
Clinical Manual for Management of the HIV-Infected ... - myCME.com

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
8–18 | <strong>Clinical</strong> <strong>Manual</strong> <strong>for</strong> <strong>Management</strong> <strong>of</strong> <strong>the</strong> <strong>HIV</strong>-<strong>Infected</strong> Adult/2006<br />
O: Objective<br />
Per<strong>for</strong>m <strong>the</strong> following tests:<br />
♦<br />
♦<br />
♦<br />
♦<br />
Check temperature and o<strong>the</strong>r vital signs, and<br />
per<strong>for</strong>m a thorough physical examination to<br />
determine potentially reversible causes such as<br />
opportunistic infections.<br />
Per<strong>for</strong>m a thorough neurologic examination,<br />
including funduscopic exam. Check symmetry<br />
<strong>of</strong> brow wrinkling, eyelid closure, and pupil size.<br />
Per<strong>for</strong>m Romberg and o<strong>the</strong>r tests to rule out focal<br />
neurologic deficits.<br />
Check gait by asking <strong>the</strong> patient to walk rapidly,<br />
turn, and stop. Ask <strong>the</strong> patient to walk on heels and<br />
tiptoes. Test steadiness <strong>of</strong> gait with eyes open and<br />
closed. Ask <strong>the</strong> patient to stand from a squatting<br />
position without assistance.<br />
Per<strong>for</strong>m a <strong>com</strong>plete minimental status examination.<br />
As a quick screen, ask <strong>the</strong> patient to write his or her<br />
name, date, and location; to spell "world" backwards;<br />
to per<strong>for</strong>m memory-object recall <strong>of</strong> 3 objects after 5<br />
minutes; and to make change from a dollar.<br />
A: Assessment<br />
Partial Differential Diagnosis<br />
♦<br />
♦<br />
♦<br />
♦<br />
O<strong>the</strong>r CNS conditions, such as toxoplasmosis,<br />
fungal infection, Mycobacterium avium <strong>com</strong>plex<br />
(MAC), lymphoma, cytomegalovirus ventriculitis<br />
or encephalitis, normal-pressure hydrocephalus,<br />
neurosyphilis, tuberculosis, or Cryptococcus<br />
neo<strong>for</strong>mans. Many <strong>of</strong> <strong>the</strong>se are treatable.<br />
Depression, which can present as cognitive<br />
impairment.<br />
O<strong>the</strong>r medical causes, such as nutritional deficiencies<br />
(eg, vitamin B12), metabolic disorders (eg,<br />
hypothyroidism), toxins (eg, chronic alcohol use), or<br />
infections (eg, tertiary syphilis)<br />
Delirium, which is an acute manifestation <strong>of</strong><br />
cognitive impairment with inability to maintain<br />
attention. Delirium can be due to many medical<br />
conditions, but is also <strong>com</strong>monly caused by<br />
medications, including those with anticholinergic<br />
adverse effects, such as amitriptyline (Elavil),<br />
promethazine (Phenergan), prochlorperazine<br />
(Compazine), and diphenhydramine (Benadryl). An<br />
anticholinergic delirium is characterized by visual<br />
or tactile hallucinations, confusion, and sometimes<br />
♦<br />
agitation. O<strong>the</strong>r medications that may cause<br />
delirium include prednisone, meperidine (Demerol),<br />
lithium (at toxic levels, which may occur in a stable<br />
patient with a serious opportunistic infection<br />
or dehydration), agonist-antagonist analgesics<br />
such as pentazocine (Talwin), and short-acting<br />
benzodiazepines such as midazolam (Versed) and<br />
triazolam (Halcion).<br />
Intoxication or withdrawal.<br />
Mild Manifestations: <strong>HIV</strong>-Associated Minor Cognitive<br />
Motor Disorder<br />
At least 2 <strong>of</strong> <strong>the</strong> following symptom should be present:<br />
♦<br />
♦<br />
♦<br />
Impaired attention, concentration, or memory<br />
Mental and psychomotor slowing<br />
Personality changes<br />
Rule out o<strong>the</strong>r causes.<br />
Severe Manifestations: <strong>HIV</strong>-Associated Dementia<br />
Signs will include <strong>the</strong> following:<br />
♦<br />
♦<br />
♦<br />
Acquired cognitive abnormality in 2 or more<br />
domains, causing functional impairment<br />
Acquired abnormality in motor per<strong>for</strong>mance or<br />
behavior<br />
No clouding <strong>of</strong> consciousness or o<strong>the</strong>r confounding<br />
cause (eg, CNS infections, psychopathology, drug<br />
abuse)<br />
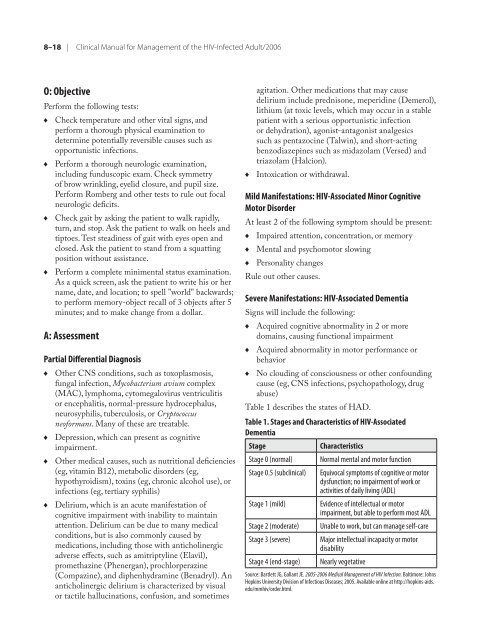
Table 1 describes <strong>the</strong> states <strong>of</strong> HAD.<br />
Table 1. Stages and Characteristics <strong>of</strong> <strong>HIV</strong>-Associated<br />
Dementia<br />
Stage Characteristics<br />
Stage 0 (normal) Normal mental and motor function<br />
Stage 0.5 (subclinical) Equivocal symptoms <strong>of</strong> cognitive or motor<br />
dysfunction; no impairment <strong>of</strong> work or<br />
activities <strong>of</strong> daily living (ADL)<br />
Stage 1 (mild) Evidence <strong>of</strong> intellectual or motor<br />
impairment, but able to per<strong>for</strong>m most ADL<br />
Stage 2 (moderate) Unable to work, but can manage self-care<br />
Stage 3 (severe) Major intellectual incapacity or motor<br />
disability<br />
Stage 4 (end-stage) Nearly vegetative<br />
Source: Bartlett JG, Gallant JE. 2005-2006 Medical <strong>Management</strong> <strong>of</strong> <strong>HIV</strong> Infection. Baltimore: Johns<br />
Hopkins University Division <strong>of</strong> Infectious Diseases; 2005. Available online at http://hopkins-aids.<br />
edu/mmhiv/order.html.














