

Clinical Manual for Management of the HIV-Infected ... - myCME.com
Clinical Manual for Management of the HIV-Infected ... - myCME.com
Clinical Manual for Management of the HIV-Infected ... - myCME.com

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
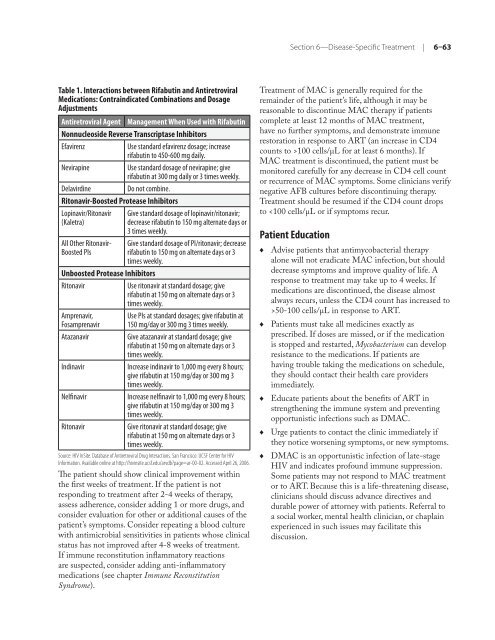
Table 1. Interactions between Rifabutin and Antiretroviral<br />
Medications: Contraindicated Combinations and Dosage<br />
Adjustments<br />
Antiretroviral Agent <strong>Management</strong> When Used with Rifabutin<br />
Nonnucleoside Reverse Transcriptase Inhibitors<br />
Efavirenz Use standard efavirenz dosage; increase<br />
rifabutin to 450-600 mg daily.<br />
Nevirapine Use standard dosage <strong>of</strong> nevirapine; give<br />
rifabutin at 300 mg daily or 3 times weekly.<br />
Delavirdine Do not <strong>com</strong>bine.<br />
Ritonavir-Boosted Protease Inhibitors<br />
Lopinavir/Ritonavir<br />
(Kaletra)<br />
All O<strong>the</strong>r Ritonavir-<br />
Boosted PIs<br />
Give standard dosage <strong>of</strong> lopinavir/ritonavir;<br />
decrease rifabutin to 150 mg alternate days or<br />
3 times weekly.<br />
Give standard dosage <strong>of</strong> PI/ritonavir; decrease<br />
rifabutin to 150 mg on alternate days or 3<br />
times weekly.<br />
Unboosted Protease Inhibitors<br />
Ritonavir Use ritonavir at standard dosage; give<br />
rifabutin at 150 mg on alternate days or 3<br />
times weekly.<br />
Amprenavir,<br />
Fosamprenavir<br />
Use PIs at standard dosages; give rifabutin at<br />
150 mg/day or 300 mg 3 times weekly.<br />
Atazanavir Give atazanavir at standard dosage; give<br />
rifabutin at 150 mg on alternate days or 3<br />
times weekly.<br />
Indinavir Increase indinavir to 1,000 mg every 8 hours;<br />
give rifabutin at 150 mg/day or 300 mg 3<br />
times weekly.<br />
Nelfinavir Increase nelfinavir to 1,000 mg every 8 hours;<br />
give rifabutin at 150 mg/day or 300 mg 3<br />
times weekly.<br />
Ritonavir Give ritonavir at standard dosage; give<br />
rifabutin at 150 mg on alternate days or 3<br />
times weekly.<br />
Source: <strong>HIV</strong> InSite. Database <strong>of</strong> Antiretroviral Drug Interactions. San Francisco: UCSF Center <strong>for</strong> <strong>HIV</strong><br />
In<strong>for</strong>mation. Available online at http://hivinsite.ucsf.edu/arvdb?page=ar-00-02. Accessed April 26, 2006.<br />
The patient should show clinical improvement within<br />
<strong>the</strong> first weeks <strong>of</strong> treatment. If <strong>the</strong> patient is not<br />
responding to treatment after 2-4 weeks <strong>of</strong> <strong>the</strong>rapy,<br />
assess adherence, consider adding 1 or more drugs, and<br />
consider evaluation <strong>for</strong> o<strong>the</strong>r or additional causes <strong>of</strong> <strong>the</strong><br />
patient’s symptoms. Consider repeating a blood culture<br />
with antimicrobial sensitivities in patients whose clinical<br />
status has not improved after 4-8 weeks <strong>of</strong> treatment.<br />
If immune reconstitution inflammatory reactions<br />
are suspected, consider adding anti-inflammatory<br />
medications (see chapter Immune Reconstitution<br />
Syndrome).<br />
Section 6—Disease-Specific Treatment | 6–63<br />
Treatment <strong>of</strong> MAC is generally required <strong>for</strong> <strong>the</strong><br />
remainder <strong>of</strong> <strong>the</strong> patient’s life, although it may be<br />
reasonable to discontinue MAC <strong>the</strong>rapy if patients<br />
<strong>com</strong>plete at least 12 months <strong>of</strong> MAC treatment,<br />
have no fur<strong>the</strong>r symptoms, and demonstrate immune<br />
restoration in response to ART (an increase in CD4<br />
counts to >100 cells/µL <strong>for</strong> at least 6 months). If<br />
MAC treatment is discontinued, <strong>the</strong> patient must be<br />
monitored carefully <strong>for</strong> any decrease in CD4 cell count<br />
or recurrence <strong>of</strong> MAC symptoms. Some clinicians verify<br />
negative AFB cultures be<strong>for</strong>e discontinuing <strong>the</strong>rapy.<br />
Treatment should be resumed if <strong>the</strong> CD4 count drops<br />
to 50-100 cells/µL in response to ART.<br />
Patients must take all medicines exactly as<br />
prescribed. If doses are missed, or if <strong>the</strong> medication<br />
is stopped and restarted, Mycobacterium can develop<br />
resistance to <strong>the</strong> medications. If patients are<br />
having trouble taking <strong>the</strong> medications on schedule,<br />
<strong>the</strong>y should contact <strong>the</strong>ir health care providers<br />
immediately.<br />
Educate patients about <strong>the</strong> benefits <strong>of</strong> ART in<br />
streng<strong>the</strong>ning <strong>the</strong> immune system and preventing<br />
opportunistic infections such as DMAC.<br />
Urge patients to contact <strong>the</strong> clinic immediately if<br />
<strong>the</strong>y notice worsening symptoms, or new symptoms.<br />
DMAC is an opportunistic infection <strong>of</strong> late-stage<br />
<strong>HIV</strong> and indicates pr<strong>of</strong>ound immune suppression.<br />
Some patients may not respond to MAC treatment<br />
or to ART. Because this is a life-threatening disease,<br />
clinicians should discuss advance directives and<br />
durable power <strong>of</strong> attorney with patients. Referral to<br />
a social worker, mental health clinician, or chaplain<br />
experienced in such issues may facilitate this<br />
discussion.














