

Clinical Manual for Management of the HIV-Infected ... - myCME.com
Clinical Manual for Management of the HIV-Infected ... - myCME.com
Clinical Manual for Management of the HIV-Infected ... - myCME.com

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>of</strong> symptoms. The risk <strong>of</strong> recurrence is higher if <strong>the</strong><br />
first depressive episode is inadequately treated or if <strong>the</strong><br />
patient has had multiple depressive episodes.<br />
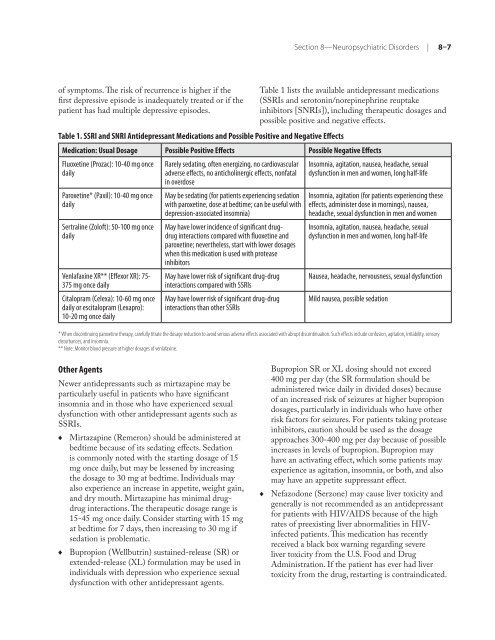
Table 1. SSRI and SNRI Antidepressant Medications and Possible Positive and Negative Effects<br />
Section 8—Neuropsychiatric Disorders | 8–7<br />
Table 1 lists <strong>the</strong> available antidepressant medications<br />
(SSRIs and serotonin/norepinephrine reuptake<br />
inhibitors [SNRIs]), including <strong>the</strong>rapeutic dosages and<br />
possible positive and negative effects.<br />
Medication: Usual Dosage Possible Positive Effects Possible Negative Effects<br />
Fluoxetine (Prozac): 10-40 mg once<br />
daily<br />
Paroxetine* (Paxil): 10-40 mg once<br />
daily<br />
Sertraline (Zol<strong>of</strong>t): 50-100 mg once<br />
daily<br />
Venlafaxine XR** (Effexor XR): 75-<br />
375 mg once daily<br />
Citalopram (Celexa): 10-60 mg once<br />
daily or escitalopram (Lexapro):<br />
10-20 mg once daily<br />
Rarely sedating, <strong>of</strong>ten energizing, no cardiovascular<br />
adverse effects, no anticholinergic effects, nonfatal<br />
in overdose<br />
May be sedating (<strong>for</strong> patients experiencing sedation<br />
with paroxetine, dose at bedtime; can be useful with<br />
depression-associated insomnia)<br />
May have lower incidence <strong>of</strong> significant drugdrug<br />
interactions <strong>com</strong>pared with fluoxetine and<br />
paroxetine; never<strong>the</strong>less, start with lower dosages<br />
when this medication is used with protease<br />
inhibitors<br />
May have lower risk <strong>of</strong> significant drug-drug<br />
interactions <strong>com</strong>pared with SSRIs<br />
May have lower risk <strong>of</strong> significant drug-drug<br />
interactions than o<strong>the</strong>r SSRIs<br />
Insomnia, agitation, nausea, headache, sexual<br />
dysfunction in men and women, long half-life<br />
Insomnia, agitation (<strong>for</strong> patients experiencing <strong>the</strong>se<br />
effects, administer dose in mornings), nausea,<br />
headache, sexual dysfunction in men and women<br />
Insomnia, agitation, nausea, headache, sexual<br />
dysfunction in men and women, long half-life<br />
Nausea, headache, nervousness, sexual dysfunction<br />
Mild nausea, possible sedation<br />
* When discontinuing paroxetine <strong>the</strong>rapy, carefully titrate <strong>the</strong> dosage reduction to avoid serious adverse effects associated with abrupt discontinuation. Such effects include confusion, agitation, irritability, sensory<br />
disturbances, and insomnia.<br />
** Note: Monitor blood pressure at higher dosages <strong>of</strong> venlafaxine.<br />
O<strong>the</strong>r Agents<br />
Newer antidepressants such as mirtazapine may be<br />
particularly useful in patients who have significant<br />
insomnia and in those who have experienced sexual<br />
dysfunction with o<strong>the</strong>r antidepressant agents such as<br />
SSRIs.<br />
♦<br />
♦<br />
Mirtazapine (Remeron) should be administered at<br />
bedtime because <strong>of</strong> its sedating effects. Sedation<br />
is <strong>com</strong>monly noted with <strong>the</strong> starting dosage <strong>of</strong> 15<br />
mg once daily, but may be lessened by increasing<br />
<strong>the</strong> dosage to 30 mg at bedtime. Individuals may<br />
also experience an increase in appetite, weight gain,<br />
and dry mouth. Mirtazapine has minimal drugdrug<br />
interactions. The <strong>the</strong>rapeutic dosage range is<br />
15-45 mg once daily. Consider starting with 15 mg<br />
at bedtime <strong>for</strong> 7 days, <strong>the</strong>n increasing to 30 mg if<br />
sedation is problematic.<br />
Bupropion (Wellbutrin) sustained-release (SR) or<br />
extended-release (XL) <strong>for</strong>mulation may be used in<br />
individuals with depression who experience sexual<br />
dysfunction with o<strong>the</strong>r antidepressant agents.<br />
♦<br />
Bupropion SR or XL dosing should not exceed<br />
400 mg per day (<strong>the</strong> SR <strong>for</strong>mulation should be<br />
administered twice daily in divided doses) because<br />
<strong>of</strong> an increased risk <strong>of</strong> seizures at higher bupropion<br />
dosages, particularly in individuals who have o<strong>the</strong>r<br />
risk factors <strong>for</strong> seizures. For patients taking protease<br />
inhibitors, caution should be used as <strong>the</strong> dosage<br />
approaches 300-400 mg per day because <strong>of</strong> possible<br />
increases in levels <strong>of</strong> bupropion. Bupropion may<br />
have an activating effect, which some patients may<br />
experience as agitation, insomnia, or both, and also<br />
may have an appetite suppressant effect.<br />
Nefazodone (Serzone) may cause liver toxicity and<br />
generally is not re<strong>com</strong>mended as an antidepressant<br />
<strong>for</strong> patients with <strong>HIV</strong>/AIDS because <strong>of</strong> <strong>the</strong> high<br />
rates <strong>of</strong> preexisting liver abnormalities in <strong>HIV</strong>infected<br />
patients. This medication has recently<br />
received a black box warning regarding severe<br />
liver toxicity from <strong>the</strong> U.S. Food and Drug<br />
Administration. If <strong>the</strong> patient has ever had liver<br />
toxicity from <strong>the</strong> drug, restarting is contraindicated.














