

Acute Leukemias - Republican Scientific Medical Library
Acute Leukemias - Republican Scientific Medical Library
Acute Leukemias - Republican Scientific Medical Library

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
146 Chapter 11 · Conventional Therapy in Adult <strong>Acute</strong> Lymphoblastic Leukemia: Review of the LALA Program<br />
into the biologic and molecular abnormalities in ALL<br />
might also provide the necessary clues that allow a<br />
clearer understanding of the crucial differences in the<br />
behavior of the different subtypes of ALL patients.<br />
11.2 General Principles<br />
In the 1960s, a major development in the treatment of<br />
ALL came from St. Jude Children’s Research Hospital<br />
in Memphis, with Don Pinkel introducing a four-phase<br />
treatment plan for ALL, what he called “Total therapy”<br />
[1] that took into account the advantage of combination<br />
chemotherapy in overcoming initial drug resistance and<br />
inhibiting acquired resistance, as well as the superiority<br />
of some drugs for remission induction and others for its<br />
continuation. All available antileukemic agents were included<br />
in the plan. The principles that were applied resulted<br />
in the regular cure of more than 50% of children<br />
with ALL. These principles were induction therapy<br />
using vincristine and prednisone, consolidation chemotherapy,<br />
a maintenance chemotherapy using 6-mercaptopurine<br />
and methotrexate, and then radiotherapy<br />
to the central nervous system (CNS) to prevent meningeal<br />
relapse. This resulted in a tremendous increase in<br />
the survival rate of patients with ALL. This regimen also<br />
recognized the importance of early intensification chemotherapy,<br />
the need for specific CNS treatment to prevent<br />
meningeal relapse, and the idea of continuing combination<br />
chemotherapy for 2 to 3 years. With this basic<br />
therapeutic strategy, results improved regularly over<br />
time with complete remission (CR) rates above 90%<br />
with recent programs and survival approaching 70–<br />
80% [2]. Unfortunately, the success that has been<br />
achieved in children with ALL has not yet been translated<br />
into adult patients [3]. Although CR rates<br />
approach now those in children, only 30–40% of adults<br />
with ALL can expect a cure 4. Less frequent than ALL in<br />
childhood, ALL in adults has long been mishandled [4,<br />
5]. The first cooperative studies in adults with ALL were<br />
initiated during the 1970s and the early 1980s [6–9], of<br />
which the first trial of the LALA group.<br />
11.3 LALA-83 Trial (1983–1985)<br />
A pilot study on 45 patients from 16 to 73 years old was<br />
initiated in 1982 to test the feasibility of an intensive and<br />
short induction phase followed by an early consolida-<br />
tion phase [10]. Eleven French centers participated to<br />
that pilot study. All patients received a 5-day course of<br />
induction chemotherapy with prednisone, vincristine,<br />
cytarabine, and rubidazone. An “AAA” regimen consisting<br />
of Adriamycin, cytarabine (Aracytine), and Asparaginase<br />
was used as consolidation. CR was achieved in<br />
73% of patients and the sequence intensive inductionearly<br />
consolidation was well tolerated and proved feasible.<br />
This allowed the development of a larger multicenter<br />
trial. The LALA-83 trial started at the beginning of<br />
1983 and ran through 1985, including 225 patients from<br />
33 French centers. The major aims of this trial were to<br />
study the usefulness of aggressive CR induction and<br />
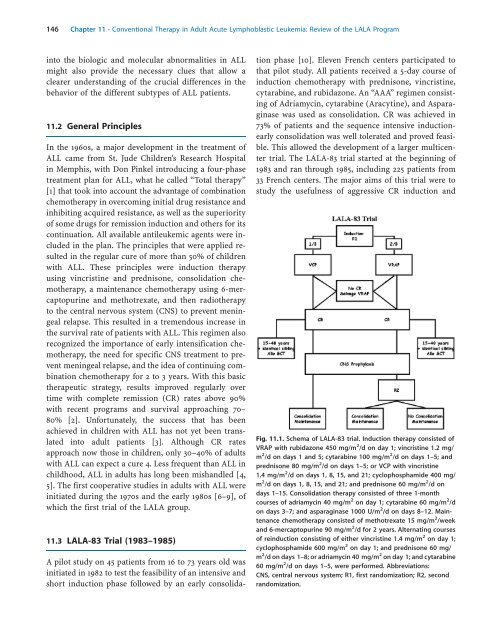
Fig. 11.1. Schema of LALA-83 trial. Induction therapy consisted of<br />
VRAP with rubidazone 450 mg/m 2 /d on day 1; vincristine 1.2 mg/<br />
m 2 /d on days 1 and 5; cytarabine 100 mg/m 2 /d on days 1–5; and<br />
prednisone 80 mg/m 2 /d on days 1–5; or VCP with vincristine<br />
1.4 mg/m 2 /d on days 1, 8, 15, and 21; cyclophosphamide 400 mg/<br />
m 2 /d on days 1, 8, 15, and 21; and prednisone 60 mg/m 2 /d on<br />
days 1–15. Consolidation therapy consisted of three 1-month<br />
courses of adriamycin 40 mg/m 2 on day 1; cytarabine 60 mg/m 2 /d<br />
on days 3–7; and asparaginase 1000 U/m 2 /d on days 8–12. Maintenance<br />
chemotherapy consisted of methotrexate 15 mg/m 2 /week<br />
and 6-mercaptopurine 90 mg/m 2 /d for 2 years. Alternating courses<br />
of reinduction consisting of either vincristine 1.4 mg/m 2 on day 1;<br />
cyclophosphamide 600 mg/m 2 on day 1; and prednisone 60 mg/<br />
m 2 /d on days 1–8; or adriamycin 40 mg/m 2 on day 1; and cytarabine<br />
60 mg/m 2 /d on days 1–5, were performed. Abbreviations:<br />
CNS, central nervous system; R1, first randomization; R2, second<br />
randomization.













