Prescription Drug Guide Comprehensive list of covered drugs
Prescription Drug Guide Comprehensive list of covered drugs
Prescription Drug Guide Comprehensive list of covered drugs
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
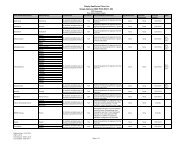
<strong>Drug</strong> Name<strong>Drug</strong>Tier Requirements/LimitsZEMAIRA INJ 1000MG 5 PA LARespiratory Tract AgentsADVAIR DISKUS AEPB 100MCG/DOSE;4 QL (60 EA per 30 days)50MCG/DOSEADVAIR DISKUS AEPB 250MCG/DOSE;4 QL (60 EA per 30 days)50MCG/DOSEADVAIR DISKUS AEPB 500MCG/DOSE;4 QL (60 EA per 30 days)50MCG/DOSEADVAIR HFA AERO 115MCG/ACT; 21MCG/ACT 4 QL (60 GM per 30 days)ADVAIR HFA AERO 230MCG/ACT; 21MCG/ACT 4 QL (60 GM per 30 days)ADVAIR HFA AERO 45MCG/ACT; 21MCG/ACT 4 QL (60 GM per 30 days)COMBIVENT AERO 103MCG/ACT; 18MCG/ACT 4DALIRESP TABS 500MCG 4ipratropium bromide/albuterol sulfate soln 2.5mg/3ml; 2 B/D MO GC0.5mg/3mlpromethazine vc syrp 5mg/5ml; 6.25mg/5ml 1 PA MO GCPULMOZYME SOLN 1MG/ML 5 PASYMBICORT AERO 160MCG/ACT; 4.5MCG/ACT 3 QL (11 GM per 30 days) MOSYMBICORT AERO 80MCG/ACT; 4.5MCG/ACT 3 QL (11 GM per 30 days) MOXOLAIR INJ 150MG 5 PA LASkeletal Muscle RelaxantsSkeletal Muscle Relaxantscarisoprodol tabs 350mg 2 PA MO GCchlorzoxazone tabs 500mg 2 PA MO GCcyclobenzaprine hcl er cp24 15mg 2 PA MO GCcyclobenzaprine hcl er cp24 30mg 2 PA MO GCcyclobenzaprine hcl tabs 10mg 2 PA MO GCcyclobenzaprine hcl tabs 5mg 2 PA MO GCmethocarbamol tabs 500mg 2 PA MO GCmethocarbamol tabs 750mg 2 PA MO GCorphenadrine citrate er tb12 100mg 2 PA MO GCorphenadrine citrate inj 30mg/ml 2 PA MO GCsoma tabs 250mg 2 MO GCtizanidine hcl caps 2mg 2 MO GCtizanidine hcl caps 4mg 2 MO GCtizanidine hcl caps 6mg 2 MO GCSleep Disorder AgentsGABA Receptor ModulatorsLUNESTA TABS 1MG 4 QL (30 EA per 30 days) STPA = Prior Authorization. ST = Step Therapy. QL = Quantity Limit. GC = Gap Coverage: We may provide coveragefor this prescription drug in the coverage gap. Please refer to our Evidence <strong>of</strong> Coverage for more information aboutthis coverage. LA = Limited Availability: This prescription may be available only at certain pharmacies. For moreinformation consult your Provider/Pharmacy Directory or call Member Services at 1-877-577-0115, 7 days a week,8:00 am – 8:00 pm Eastern. TTY/TDD users should call 711. MO = Mail Order: This prescription may be availablethrough mail-order service, please refer to our Evidence <strong>of</strong> Coverage for more information. ED = Excluded <strong>Drug</strong>: Thisprescription drug is not normally <strong>covered</strong> in a Medicare <strong>Prescription</strong> <strong>Drug</strong> Plan. However, Simply Healthcare Plans,Inc. does provide supplemental coverage for these medications. The amount you pay when you fill a prescription forthis drug does not count towards your total drug costs (that is, the amount you pay does not help you qualify forcatastrophic coverage). In addition, if you are receiving extra help to pay for your prescriptions, you will not get anyextra help to pay for this drug. Page 95