Prescription Drug Guide Comprehensive list of covered drugs
Prescription Drug Guide Comprehensive list of covered drugs
Prescription Drug Guide Comprehensive list of covered drugs
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
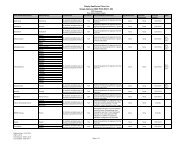
<strong>Drug</strong> Name<strong>Drug</strong>Tier Requirements/Limitslevoxyl tabs 100mcg 1 MO GClevoxyl tabs 112mcg 1 MO GClevoxyl tabs 125mcg 1 MO GClevoxyl tabs 137mcg 1 MO GClevoxyl tabs 150mcg 1 MO GClevoxyl tabs 175mcg 1 MO GClevoxyl tabs 200mcg 1 MO GClevoxyl tabs 25mcg 1 MO GClevoxyl tabs 50mcg 1 MO GClevoxyl tabs 75mcg 1 MO GClevoxyl tabs 88mcg 1 MO GCliothyronine sodium tabs 25mcg 1 MO GCliothyronine sodium tabs 50mcg 1 MO GCliothyronine sodium tabs 5mcg 1 MO GCSYNTHROID TABS 100MCG 3 MOSYNTHROID TABS 112MCG 3 MOSYNTHROID TABS 125MCG 3 MOSYNTHROID TABS 137MCG 3 MOSYNTHROID TABS 150MCG 3 MOSYNTHROID TABS 175MCG 3 MOSYNTHROID TABS 200MCG 3 MOSYNTHROID TABS 25MCG 3 MOSYNTHROID TABS 300MCG 3 MOSYNTHROID TABS 50MCG 3 MOSYNTHROID TABS 75MCG 3 MOSYNTHROID TABS 88MCG 3 MOTIROSINT CAPS 100MCG 4TIROSINT CAPS 112MCG 4TIROSINT CAPS 125MCG 4TIROSINT CAPS 137MCG 4TIROSINT CAPS 25MCG 4TIROSINT CAPS 50MCG 4TIROSINT CAPS 75MCG 4TIROSINT CAPS 88MCG 4unithroid tabs 100mcg 1 MO GCunithroid tabs 112mcg 1 MO GCunithroid tabs 125mcg 1 MO GCunithroid tabs 150mcg 1 MO GCPA=Autorización previa. ST=Terapia por fases. QL=Límite en la Cantidad. GC=Es posible que proporcionemoscobertura adicional de este medicamento recetado durante la brecha en la cobertura. Consulte nuestra Evidencia deCobertura para obtener más información sobre esta cobertura. GC D = Cobertura adicional durante la brecha para ciertoplanes. LA=Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información,consulte su Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115. Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios conTTY/TDD deben marcar 711. MO=Este medicamento recetado puede obtener mediante pedido por correo. ED=Estemedicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare. Lacantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total demedicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástr<strong>of</strong>e).Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayudaadicional para pagar este medicamento. Page 82