Prescription Drug Guide Comprehensive list of covered drugs
Prescription Drug Guide Comprehensive list of covered drugs
Prescription Drug Guide Comprehensive list of covered drugs
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
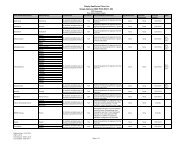
<strong>Drug</strong> Name<strong>Drug</strong>Tier Requirements/LimitsPANCREAZE CPEP 70000UNIT; 16800UNIT; 440000UNITZAVESCA CAPS 100MG 5ZENPEP CPEP 109000UNIT; 20000UNIT; 68000UNIT 3 MOZENPEP CPEP 136000UNIT; 25000UNIT; 85000UNIT 3 MOZENPEP CPEP 27000UNIT; 5000UNIT; 17000UNIT 3 MOZENPEP CPEP 55000UNIT; 10000UNIT; 34000UNIT 3 MOZENPEP CPEP 82000UNIT; 15000UNIT; 51000UNIT 3 MOEnzyme Replacement/ModifiersEnzyme Replacement/ModifiersPERTZYE CPEP 30250UNIT; 8000UNIT; 28750UNIT 4 MOPERTZYE CPEP 60500UNIT; 16000UNIT; 57500UNIT 4 MOVIOKACE TABS 39150UNIT; 10440UNIT; 39150UNIT 4 MOVIOKACE TABS 78300UNIT; 20880UNIT; 78300UNIT 4 MOGastrointestinal AgentsAntispasmodics, Gastrointestinaldicyclomine hcl caps 10mg 1 PA MO GCdicyclomine hcl soln 10mg/5ml 1 PA MO GCdicyclomine hcl tabs 20mg 1 PA MO GCglycopyrrolate inj 0.2mg/ml 1 MO GCglycopyrrolate tabs 1mg 2 MO GCglycopyrrolate tabs 2mg 2 MO GCmethscopolamine bromide tabs 2.5mg 2 MO GCmethscopolamine bromide tabs 5mg 2 MO GCGastrointestinal Agents, OtherCHENODAL TABS 250MG 5diphenoxylate/atropine liqd 0.025mg/5ml; 2.5mg/5ml 1 PA MO GCdiphenoxylate/atropine tabs 0.025mg; 2.5mg 1 PA MO GCloperamide hcl caps 2mg 1 MO GCRELISTOR INJ 12MG/0.6ML 4 QL (18 EA per 30 days) PAursodiol caps 300mg 1 MO GCGastrointestinal Agentsgavilyte-c solr 240gm; 2.98gm; 6.72gm; 5.84gm; 1 MO GC22.72gmgavilyte-g solr 236gm; 2.97gm; 6.74gm; 5.86gm; 1 MO GC22.74gmgavilyte-n/flavor pack solr 420gm; 1.48gm; 5.72gm; 1 MO GC11.2gmHELIDAC MISC 0; 0; 0 4 QL (56 EA per 30 days)PA = Prior Authorization. ST = Step Therapy. QL = Quantity Limit. GC = Gap Coverage: We may provide coveragefor this prescription drug in the coverage gap. Please refer to our Evidence <strong>of</strong> Coverage for more information aboutthis coverage. LA = Limited Availability: This prescription may be available only at certain pharmacies. For moreinformation consult your Provider/Pharmacy Directory or call Member Services at 1-877-577-0115, 7 days a week,8:00 am – 8:00 pm Eastern. TTY/TDD users should call 711. MO = Mail Order: This prescription may be availablethrough mail-order service, please refer to our Evidence <strong>of</strong> Coverage for more information. ED = Excluded <strong>Drug</strong>: Thisprescription drug is not normally <strong>covered</strong> in a Medicare <strong>Prescription</strong> <strong>Drug</strong> Plan. However, Simply Healthcare Plans,Inc. does provide supplemental coverage for these medications. The amount you pay when you fill a prescription forthis drug does not count towards your total drug costs (that is, the amount you pay does not help you qualify forcatastrophic coverage). In addition, if you are receiving extra help to pay for your prescriptions, you will not get anyextra help to pay for this drug. Page 69