Prescription Drug Guide Comprehensive list of covered drugs
Prescription Drug Guide Comprehensive list of covered drugs
Prescription Drug Guide Comprehensive list of covered drugs
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
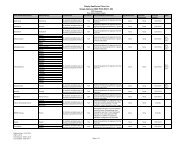
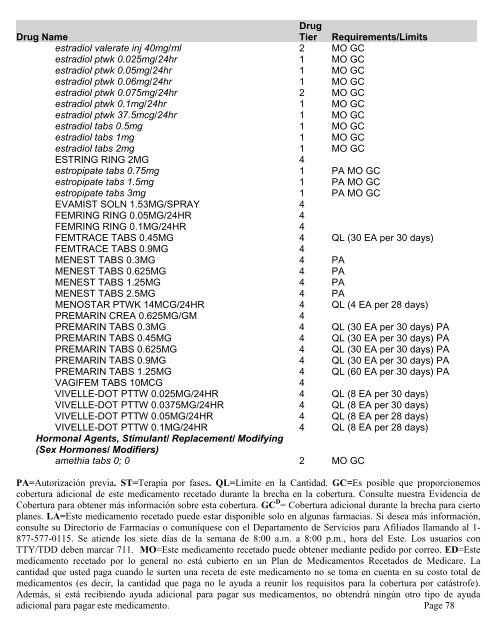
<strong>Drug</strong> Name<strong>Drug</strong>Tier Requirements/Limitsestradiol valerate inj 40mg/ml 2 MO GCestradiol ptwk 0.025mg/24hr 1 MO GCestradiol ptwk 0.05mg/24hr 1 MO GCestradiol ptwk 0.06mg/24hr 1 MO GCestradiol ptwk 0.075mg/24hr 2 MO GCestradiol ptwk 0.1mg/24hr 1 MO GCestradiol ptwk 37.5mcg/24hr 1 MO GCestradiol tabs 0.5mg 1 MO GCestradiol tabs 1mg 1 MO GCestradiol tabs 2mg 1 MO GCESTRING RING 2MG 4estropipate tabs 0.75mg 1 PA MO GCestropipate tabs 1.5mg 1 PA MO GCestropipate tabs 3mg 1 PA MO GCEVAMIST SOLN 1.53MG/SPRAY 4FEMRING RING 0.05MG/24HR 4FEMRING RING 0.1MG/24HR 4FEMTRACE TABS 0.45MG 4 QL (30 EA per 30 days)FEMTRACE TABS 0.9MG 4MENEST TABS 0.3MG 4 PAMENEST TABS 0.625MG 4 PAMENEST TABS 1.25MG 4 PAMENEST TABS 2.5MG 4 PAMENOSTAR PTWK 14MCG/24HR 4 QL (4 EA per 28 days)PREMARIN CREA 0.625MG/GM 4PREMARIN TABS 0.3MG 4 QL (30 EA per 30 days) PAPREMARIN TABS 0.45MG 4 QL (30 EA per 30 days) PAPREMARIN TABS 0.625MG 4 QL (30 EA per 30 days) PAPREMARIN TABS 0.9MG 4 QL (30 EA per 30 days) PAPREMARIN TABS 1.25MG 4 QL (60 EA per 30 days) PAVAGIFEM TABS 10MCG 4VIVELLE-DOT PTTW 0.025MG/24HR 4 QL (8 EA per 30 days)VIVELLE-DOT PTTW 0.0375MG/24HR 4 QL (8 EA per 30 days)VIVELLE-DOT PTTW 0.05MG/24HR 4 QL (8 EA per 28 days)VIVELLE-DOT PTTW 0.1MG/24HR 4 QL (8 EA per 28 days)Hormonal Agents, Stimulant/ Replacement/ Modifying(Sex Hormones/ Modifiers)amethia tabs 0; 0 2 MO GCPA=Autorización previa. ST=Terapia por fases. QL=Límite en la Cantidad. GC=Es posible que proporcionemoscobertura adicional de este medicamento recetado durante la brecha en la cobertura. Consulte nuestra Evidencia deCobertura para obtener más información sobre esta cobertura. GC D = Cobertura adicional durante la brecha para ciertoplanes. LA=Este medicamento recetado puede estar disponible solo en algunas farmacias. Si desea más información,consulte su Directorio de Farmacias o comuníquese con el Departamento de Servicios para Afiliados llamando al 1-877-577-0115. Se atiende los siete días de la semana de 8:00 a.m. a 8:00 p.m., hora del Este. Los usuarios conTTY/TDD deben marcar 711. MO=Este medicamento recetado puede obtener mediante pedido por correo. ED=Estemedicamento recetado por lo general no está cubierto en un Plan de Medicamentos Recetados de Medicare. Lacantidad que usted paga cuando le surten una receta de este medicamento no se toma en cuenta en su costo total demedicamentos (es decir, la cantidad que paga no le ayuda a reunir los requisitos para la cobertura por catástr<strong>of</strong>e).Además, si está recibiendo ayuda adicional para pagar sus medicamentos, no obtendrá ningún otro tipo de ayudaadicional para pagar este medicamento. Page 78