Prescription Drug Guide Comprehensive list of covered drugs
Prescription Drug Guide Comprehensive list of covered drugs
Prescription Drug Guide Comprehensive list of covered drugs
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
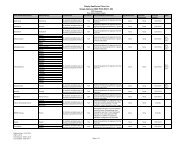
<strong>Drug</strong> Name<strong>Drug</strong>Tier Requirements/LimitsGOLYTELY SOLR 236GM; 2.97GM; 6.74GM; 5.86GM; 422.74GMHALFLYTELY BOWEL PREP/FLAVOR PACKS KIT 45MG; 210GM; 0.74GM; 2.86GM; 5.6GMKRISTALOSE PACK 10GM 4 MOKRISTALOSE PACK 20GM 4 MOlactulose soln 10gm/15ml 1 MO GCMOVIPREP SOLR 4.7GM; 100GM; 1.015GM; 5.9GM; 42.691GM; 7.5GMpolyethylene glycol 3350 powd 0 1 MO GCProtectantsCARAFATE SUSP 1GM/10ML 4misoprostol tabs 100mcg 2misoprostol tabs 100mcg 2misoprostol tabs 100mcg 2misoprostol tabs 100mcg 2misoprostol tabs 200mcg 1 MO GCsucralfate tabs 1gm 1 MO GCProton Pump InhibitorsDEXILANT CPDR 30MG 4 QL (30 EA per 30 days) STDEXILANT CPDR 60MG 4 QL (30 EA per 30 days) STlansoprazole cpdr 15mg 2 QL (30 EA per 30 days) MO GClansoprazole cpdr 30mg 2 QL (30 EA per 30 days) MO GCNEXIUM I.V. INJ 20MG 4NEXIUM I.V. INJ 40MG 4NEXIUM CPDR 20MG 3 QL (30 EA per 30 days) MONEXIUM CPDR 40MG 3 QL (30 EA per 30 days) MONEXIUM PACK 10MG 3 QL (30 EA per 30 days) MONEXIUM PACK 20MG 3 QL (30 EA per 30 days) MONEXIUM PACK 40MG 3 QL (30 EA per 30 days) MOomeprazole cpdr 10mg 1 MO GComeprazole cpdr 20mg 1 MO GComeprazole cpdr 40mg 1 MO GCpantoprazole sodium tbec 20mg 1 MO GCpantoprazole sodium tbec 40mg 1 MO GCGenitourinary AgentsAntispasmodics, UrinaryDETROL LA CP24 2MG 4 QL (30 EA per 30 days)DETROL LA CP24 4MG 4 QL (30 EA per 30 days)PA = Prior Authorization. ST = Step Therapy. QL = Quantity Limit. GC = Gap Coverage: We may provide coveragefor this prescription drug in the coverage gap. Please refer to our Evidence <strong>of</strong> Coverage for more information aboutthis coverage. LA = Limited Availability: This prescription may be available only at certain pharmacies. For moreinformation consult your Provider/Pharmacy Directory or call Member Services at 1-877-577-0115, 7 days a week,8:00 am – 8:00 pm Eastern. TTY/TDD users should call 711. MO = Mail Order: This prescription may be availablethrough mail-order service, please refer to our Evidence <strong>of</strong> Coverage for more information. ED = Excluded <strong>Drug</strong>: Thisprescription drug is not normally <strong>covered</strong> in a Medicare <strong>Prescription</strong> <strong>Drug</strong> Plan. However, Simply Healthcare Plans,Inc. does provide supplemental coverage for these medications. The amount you pay when you fill a prescription forthis drug does not count towards your total drug costs (that is, the amount you pay does not help you qualify forcatastrophic coverage). In addition, if you are receiving extra help to pay for your prescriptions, you will not get anyextra help to pay for this drug. Page 71