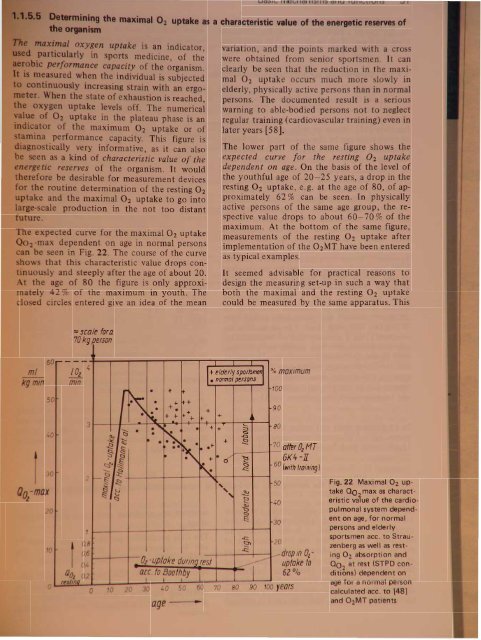
m 1m I O2 uptake a a characteristic value of the energetic r rv of~_I%il,"tli 0 ygen uptake i an indicatorpaJrtic:ulllrl in port medicine, of th~formance capacity of the organism.mElaslued hen the individual is subjectedCOlfttiftuously increasing train with an ergo-~2.ner. n tate of exhau tion is reached,uptake levels off. The numericaluptake in the plateau phase is anof the maximum 02 uptake or ofp rformance capacity. This figure isGl8l1Jlosti ally very informative, as it can also1n a a ind of characteristic value of the"j~"etic reserves of the organism. It wouldtheltet-ore be desirable for measurement devicesroutine determination of the resting O2uJ)'talc:e and the maximal O2 uptake to go into- cale production in the not too distante pected curve for the maximal O2 uptake2 -rna dependent on age in normal personsbe een in Fig. 22. The course of the curveo that this characteristic value drops con-. uou ly and steeply after the age of about 20.the age of 80 the figure is only approxirnaely 42 % of the maximum in youth. Thec osed circles entered give an idea of the meanvariation, and the points marked with a crowere obtained from enior sportsmen. It canclearly be seen that the reduction in the maximalO2 uptake occurs much more slowly inelderly, physically active persons than in normalpersons. The documented result is a seriouswarning to able-bodied persons not to neglectregular training (cardiovascular training) even inlater years [58].The lower part of the same figure shows theexpected curve for the resting O 2 uptakedependent on age. On the basis of the level ofthe youthful age of 20-25 years, a drop in theresting O2 uptake, e.g. at the age of 80, of approximately62 % can be seen. In physicallyactive persons of the same age group, the respectivevalue drops to about 60-70 % of themaximum. At the bottom of the same figure,measurements of the resting O2 uptake afterimplementation of the 02MT have been enteredas typical examples.It seemed advisable for practical reasons todesign the measuring set-up in such a way thatboth the maximal and the resting O2 uptakecould be measured by the same apparatus. Thismtkgmm~-max6050o302010----=scale fora70 kg persontOz 4 I+elderly SPorfsme1 % maximum• normal personsmin10o3r~ • + ft• ++ +++• • +90• +~+ + + + +-,.~ • + + ::::s 80Ci • Q•-Q~ ..... it •~~+ ~~ ~ •• Ie .+70 afler OzMT§- §•6K4-JI~'" ~ t:::i 60~ .0' ~.c:(wtfh training)~C;)'-~2§ ~ 501a, . ,~ ~ ~c::J "~ 40~ QE:300,8 c:::J\0,6dropm Ozuptake10Ol-uptake durmg/est ---ace to Boothby62%0,4---I,.,, ~rfnQ 0.2I I Io 10 20 30 40 50 60 70 80 90 100 yeorsage-..c:::..c:::20Fig.22 Maximal 02 uptakeQO max as characteristicva~ue of the cardiopulmonalsystem dependenton age, for normalpersons and elderlysportsmen ace. to Strauzenbergas well as restingO2 absorption and00 2at rest (STPD con·ditions) dependent onage for a normal personcalculated ace. to (48]and 02MT patients
hi v d in h arrangement shown aboveby th u of a flow sen or covering the rangefr m 0.12 to 20 1/ . In addition, the flow channelswere designed with an inner diameter ofmore than 20 mm in order to keep the flowresistance sufficiently low, even in flow peaks.1.1.&.Determining the lung function parametersPn umologists (Petro, Daum) were, as quoted Case I:in (17), of the opinion that the oxygen multiteptherapy procedures could not bring abouta lasting improvement of the parameters of lungfunction [59): 'None of these partial functionsof respiration can be changed in any way by theexogenous supply of oxygen'. This standpointwas opposed by the author's expectation that,by means of the high-charging of the bloodmicrocirculation in the lung area also, and thelasting improvement in the energetic status (anincrease in the performance capacity of therespiratory musculature), a long-term improvementin the parameters of lung function does orcan occur. In order to settle this question apilot study was performed, at first by DrGabriele Caspers and finally by us. For this aSpiroton-2 device from the Dragerwerk, LUbeck,FRG, was used, made available by the courtesyof the Erwin Braun Institute of PreventiveMedicine, Engelberg, Switzerland. This instrumentdetermines from a single expiratorybreath, which can be repeated twice after anadequate interval, the parameters exemplifiedin the two following cases. The parameters areretrieved from a memory and are evaluated insidethe instrument. The results are presentedby a plotter as flow and volume/time curves. Inthis way the following results were documented,showing that lasting improvements in lung parametersdue to oxygen multistep therapy reallycan be objectified (see column, right).In 15 patients from our group we found an increaseof 6.5 % in the vital capacity and of15.4 % in the peak flow (PF) after 02MT.Peak flow[1. S-I]FVC [1]FEV 1 [1]24-year-old male patient with functionalvegetative complaints. Treatment:two 15 min O:zMT quick proceduresDifferenceParameter before after abso. relativeO:zMT lutePeak flow[I'S-l]FVC [1]FEVI [1]Case 2:8.215.274.284.683.391.8710.506.044.265.813.602.08Explanation of the abbreviations:+ 2.29+ 0.77- 0.02+ 28%+ 15%0%54-year-old male patient with obstructiveventilation disorder. Treatment:36 h 18 day O:zMT procedureDifferenceParameter before after abso:- relative02MT lute+ 1.13 + 24%+ 0.21+ 0.21+ 6%+ 11%- Peak flow = maximum expiratory flow- FVC = forced vital capacity (in maximumexpiration)= l-second forced expiratory volume;Tiffeneau testDr Gabriele Caspers also produced similarlypositive findings with improvement in these andfurther lung parameters on 171 patients in theKlinik fiir Naturheilverfahren, Bad FUssing,FRG [60, 400a].1.1.6.7 Determining the resting CO 2 production as a characteristic value of the oxygen utilized bythe organismIn order to be able to differentiate the metabolicpathways of the (additionally) absorbedoxygen in the organism, it is also necessary todetermine quantitatively the C02 emission ofth lung. igure 23 show a schematic pictureof the e pathways. The ab orbed oxygen i u edfor energy production (biological oxidation)in the re piratory chain of the mitochondria ofall cell . Part of the energy gained is requiredfor imrnun proce es, detoxification reaction ,in hormone syntheses and in protein metabolism.The C02 production per unit of time O' min -1)can be determined by measurement of thabsolute CO2 content of the expiration air.Information about the oxygen actually convertedin the organism can thu b obtained bmea uring the O2 mi ion. Th ignifi anof this paramet r i ubj ct to thre limit ti nhow ver:
- Page 1 and 2: sand functl ni ove d cellular capil
- Page 3: 8 1. Physiological fou~dationsmmHga
- Page 6 and 7: Basic mechanisms and functions 11e
- Page 8 and 9: Basic mechanisms and functions 13pr
- Page 11 and 12: 500r-T_-+5__r-_-+1O__,....-_~15.1O-
- Page 13 and 14: ~IUI1!J ~atpWorMs---~~·tIIlDkeJ \I
- Page 15 and 16: y r na onabS,olu'te clla.ra~t ri ti
- Page 17 and 18: 100907065"I 4y iological foundation
- Page 19 and 20: 1. hy lologlcal foundations70"''''J
- Page 21 and 22: CII'Cli8LC outl)ut VAr;lllil i e re
- Page 23 and 24: -'0 y 101091cai oundatlons80%6050l~
- Page 25: ,..._........,.--~"'!""!!'!~~----_.
- Page 29 and 30: 34 1. Physiological foundations70%6
- Page 31 and 32: logical foundationsu .on in the opt
- Page 33 and 34: 1. Physiological foundations. ~ la~
- Page 35 and 36: II foundationsI tem IBPtrsons with
- Page 37: 1. Physiological foundationsAirdosi
- Page 40 and 41: 110N.ttJJOt~1. Physiological founda
- Page 42 and 43: 1. Phy iological foundationsAnoO;HT
- Page 44 and 45: hysiological foundations...fJJHT(JI
- Page 46 and 47: 1. Physiological foundationsCOCOM I
- Page 48 and 49: g r d, whi h con iderably contribut
- Page 50 and 51: logical foundations13IrPtz12.......
- Page 52 and 53: ,. Physiological foundationsIf-RoN
- Page 54 and 55: 1. Physiological foundationsAll"i1t
- Page 56 and 57: ~~itItINitIIJq/s N 31 54 52~IBIP~-.
- Page 58 and 59: BDuring OzMTprocedurecAfter OzMTpro
- Page 60 and 61: A Bi3lrfss 1'1oafofmovement 8 0pl'r
- Page 62 and 63: Table 6 PO b measurements of unsele
- Page 64 and 65: serert~ hyperoxia pure 0 } .distres
- Page 66 and 67: IIstress qirI/iII mn wryhJI1IJSISLo
- Page 68 and 69: A/JtfJtnk«P~1Mtrr'ttriIWIItJfIS~.~
- Page 70 and 71: Table 7 The change in the architect
- Page 72 and 73: nsMslor rotd'1uI.-Jl!Jg1"/11(J(Jrfr
- Page 74 and 75: IonsFig. 74 Histological pictures s
- Page 76 and 77:
IonseM' Selecfofherm equipment-_s1S
- Page 78 and 79:
.....-------................',..,-n
- Page 80 and 81:
eM/rot gro"/!.Histologicallyconfirm
- Page 82 and 83:
A1er tnit,almonipulotionsand III«l
- Page 84 and 85:
Q'CSlNltftning1A. QfQ/-fJlf1inguQ
- Page 86 and 87:
otllm'lv.2 h th ju tifi d pro p ct
- Page 88 and 89:
t48xlD J WsEhmmahooofMe ~crdieal, c
- Page 90 and 91:
old°z-/ImitMW mode of calcu/aflonC
- Page 92 and 93:
he cylindr'cal area upplied by the'
- Page 94 and 95:
Tn-T-~-----1~--~--~JaluralttJtranSi
- Page 96 and 97:
aPI)Ii:lcati?n with a patially very
- Page 98 and 99:
are triggered. At the same site, ho
- Page 100 and 101:
n respired again, the drop in respi
- Page 102 and 103:
Exholationtubeloop aroundcmebroncll
- Page 104 and 105:
[Xeftt of,t"". Respiratorv... stand
- Page 106 and 107:
ventieFig. 112 pH decrease between
- Page 108 and 109:
BIncorporation ofJ5s-slI"ate intofh
- Page 110 and 111:
~LFig. 115 Electron micrograph of h
- Page 112 and 113:
12111098V ~ .-"~"' .....b""", ".1Tt
- Page 114 and 115:
,,,;tt cola;, ofH1e 88JIJitKIJIIl "
- Page 116 and 117:
"-1r-180 I'\112007(J)Jr' '- jwry¥I