Basic mechanisms and functions 13produced (02MT procedure with high O 2offero the lungt adapted to the respiration minutevolume RMV) and when there is a high capillary~lood flow Q (high cardiac output tphysicale. erbo~). The strength of the blood microclrCula.tlOn.therefore plays a significant role inthe tr~ggen!"g of the switching mechanism oft~e mIcrocirculation. The reason why a reduc~lon o~ the microcirculation (cardiac infarction,mtermltt~nt claudication) occurs more fre~uently. m older persons may be considered tohe ?artlcularly in the decrease in the nutritivecapl1la~ blood flow (reduction of cardiac outputwith age [37]) and thereby in the Po 2·ven·According to these explanations the scale ofthe resting P0 2 of the various o~gans and tissues(Fig. S B) gives us a clue to the mean riskfor the various organs and tissues in O 2 deficiency(old. age [37]t. stressful influences [20, 21].Accordmg to thIS compromise of the heart(myocardiac infarction) could first be expectedin O2 deficiency, due to diminishing of themicrocirculation, and then in the lower extremities,and also in the brain (circulatorydisorders, dizziness) and in the eyes. Correspondinglyit is to be expected that an improvementof the O 2 status with procedurevariants of the oxygen multistep therapy orstamina training, will help first the heart, thenthe lower extremities, as well as the brain(circulatory disorders) and the eyes. The aboveformulated rules give us new insights into themultifactorial process in various importantdiseases, suffering and complaints based onO 2 deficiency.Due to the discovered correlation between thequality of the O 2 status and the strength of theho t's cellular defense capacity [18], significantlocal differences in the strength of the defensecapacity dependent on location, can be expectedin the human organism from this viewpoint.Thi assessment carries more weightwhen we begin to take into account the localvariations in the defense cell density (differencesin the parameters of the capillary networkand the microcirculation etc.). Cancertumors can be expected to manifest themselvesmore frequently in parts of the organism wherelocal minima in the O2 status and in the defensecell den ity have existed over a certain periodof time. It i particularly easy to recognize 02tatu minima in the area of the skin, e.g. bymean of tran cutaneou large area measurementof th P02' Skin abnormalitie often formth ground of uch minima, which can bemade to di ppear or at lea t to weaken byo ygen multi tep timulation of the ho t'defense. Investigations of this type lead to aninteresting dermatological research area.The peripheral circulatory disorders in thelower extremities, caused by a deterioration inthe O2 status and often ending in the necessityof a leg amputation, are among the commonestillnesses of old age. This fact can be explainedby the low level of the resting P0 2 - ven measuredin a standing position, of this area of the skeletalmusculature, already discussed (see also Fig.S B), combined with the drop in the resting O2uptake of the organism, or of the cardiac output,to a level at the age of 75 years of 65 % or62 %, relative to the maximum (30 years).In order to round off our ideas, it seemed necessaryto find an answer to the question of whythis disease affects primarily the lower, and notthe upper, extremities, and why O2 multisteptherapy (and also HOT-UVR therapy) usuallygives unique aid particularly in circulatory disordersof the lower extremities (Fig. S A). Inorder to answer these questions, measurementsof the resting P0 2 • ven at the upper and lowerextremities were undertaken, in a standing position,the mean levels of which can be found inFig. S B. As our ideas had led us to expect, itwas found that the venous resting P02 in thelower extremity is significantly lower that inthe upper (measurement in a tanding po ition),by 7 mmHgjO.93 kPa). This result explain thepreference of the lower extremities in thepathogenic decharging of the microcirculationin the skeletal musculature, and in the therapeutichigh-charging.Within the framework of these investigationwe gained information about the cour e of thevenous resting P0 2 and the blood microcirculationin the lower extremities during the pathogenicand therapeutic proces es, ummarized inFig. 6. It may eem di concerting at first that apoor O2 supply to the capillary wall cell canexist with a high level of the local mixed P0 2 - ven(Fig. 6 C) and conversely, that the be t O 2supply (Fig. 6 E) can occur with a parti ularlylow level of the local mixed p0 2 • ven ' The eparadoxical findings can be explained b achange in the diffusion area a a function ofthe nutritive blood flow Q, whi h i er low inthe fir t ca e and very high in the e ond ( eealso the abov relation hip of the effe tivenof 02MT procedure). The dynami of thmicrocirculation al 0 contribute to th fa tthat, in th P0 2 - ven control of th di 0 r dwitching m chani m, the Po 2 - en 1 el f thwitching thr hold for th low ring r rai ingof th mi rocir ulation ar ery far apart (Fig.6, right).
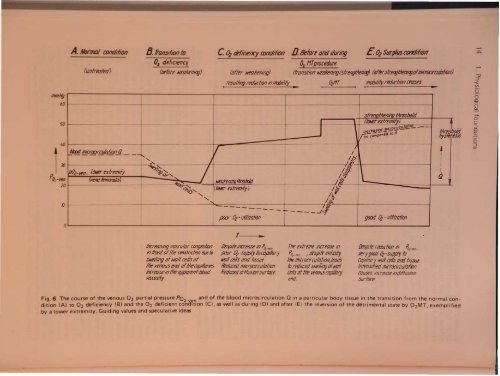
~~6050~NtJnnoI aJntiilion(un/mImi)8.1rJtuition to0, deficiency(/rfore IVl'fJIfeRlng)c. ~ ti'fI~IK''y trJIltltliJn D.lkfortandtlunilg0, MTprocedure(after IlIf(JRenlilg)-- -----Eo ~ SurplusantiI!iJRftransilton MtNnil1l)/slrengllM'l1ilf) (Of/wslr~t!ll'nigofmi7ocituloliJn)rt'Sulltng mluelmn tm7/uly {}z1fT mollllily mue/ionct't1Sl'SI .. I I ...... , -....:.-----strmol!leninJ flnsllfJld._- 1 (/0It'e!"extll'mity)increas'!- - 7' A;;;C;;'pared Dd mlcrDClfe!!Jt!!1."'J---6bxiIIICnx:1ffi1'otion f1 rrI ,I~---------I"/6'I ~I~JJ.'~~"'/,~ II pOz-vm, 10000exlmnlly ~....... IIIq.."(WI1ll fmK¥rJIis)If)~l\et1/(eni/lOIImIKidLQP Or "",~::r,:-.(Ii»Itr !X/remilft /~...q.~:-...20IKJV' ..............,/~IIf------- I~- - - - -..I':J~PJOr l??- utilizationot ...g«Xi Oz -utIlizationg~~'O!tI~~""U:r-< VIoc.o(')Q)-+.oC:::J0.Q)-o:::JVIincreasIng I/osculor congesliJnin fronlofIlle constridiOll due toslVt'lltilg ofMIllcells ot1m- venous endoflitetlljl/llories#7mrlselilllletI,IJ,lJoll'ntIJItxJdviscosity..De~/e /i7t:rease til Parrenjloor 0 sUjlPIy toco,oi/laryIt'llilcells tlnd lissue.Reduced micrOCIrculation.HeduceddiffUSIOnsurface,The extreme increase in!'orren I despite intliallylow microcirculafion,lfodsto reriuced swelllflgofwallailsof the reflOUS cuplilor]end.Despite rl'duetm ,n ~-ren.verygood 0;-Slippl1 toCll,tJlllary wollcrlls anti tIssue.intenSIfied mlcr(){Yrculaloncauses Increase mitffuSIOnSUrloce.Fig.6 The course of the venous 02 partial pressure P02-v and of the blood microcirculation Q in a particular body tissue in the transition from the normal condition(A) to 02 deficiency (B) and the 02 deficient cona~~on (e), as well as during (0) and after (E) the reversion of the detrimental state by 02MT, exemplifiedby a lower extremity. Guiding values and speculative ideas
- Page 1 and 2: sand functl ni ove d cellular capil
- Page 3: 8 1. Physiological fou~dationsmmHga
- Page 6 and 7: Basic mechanisms and functions 11e
- Page 11 and 12: 500r-T_-+5__r-_-+1O__,....-_~15.1O-
- Page 13 and 14: ~IUI1!J ~atpWorMs---~~·tIIlDkeJ \I
- Page 15 and 16: y r na onabS,olu'te clla.ra~t ri ti
- Page 17 and 18: 100907065"I 4y iological foundation
- Page 19 and 20: 1. hy lologlcal foundations70"''''J
- Page 21 and 22: CII'Cli8LC outl)ut VAr;lllil i e re
- Page 23 and 24: -'0 y 101091cai oundatlons80%6050l~
- Page 25 and 26: ,..._........,.--~"'!""!!'!~~----_.
- Page 27 and 28: hi v d in h arrangement shown above
- Page 29 and 30: 34 1. Physiological foundations70%6
- Page 31 and 32: logical foundationsu .on in the opt
- Page 33 and 34: 1. Physiological foundations. ~ la~
- Page 35 and 36: II foundationsI tem IBPtrsons with
- Page 37: 1. Physiological foundationsAirdosi
- Page 40 and 41: 110N.ttJJOt~1. Physiological founda
- Page 42 and 43: 1. Phy iological foundationsAnoO;HT
- Page 44 and 45: hysiological foundations...fJJHT(JI
- Page 46 and 47: 1. Physiological foundationsCOCOM I
- Page 48 and 49: g r d, whi h con iderably contribut
- Page 50 and 51: logical foundations13IrPtz12.......
- Page 52 and 53: ,. Physiological foundationsIf-RoN
- Page 54 and 55: 1. Physiological foundationsAll"i1t
- Page 56 and 57: ~~itItINitIIJq/s N 31 54 52~IBIP~-.
- Page 58 and 59:
BDuring OzMTprocedurecAfter OzMTpro
- Page 60 and 61:
A Bi3lrfss 1'1oafofmovement 8 0pl'r
- Page 62 and 63:
Table 6 PO b measurements of unsele
- Page 64 and 65:
serert~ hyperoxia pure 0 } .distres
- Page 66 and 67:
IIstress qirI/iII mn wryhJI1IJSISLo
- Page 68 and 69:
A/JtfJtnk«P~1Mtrr'ttriIWIItJfIS~.~
- Page 70 and 71:
Table 7 The change in the architect
- Page 72 and 73:
nsMslor rotd'1uI.-Jl!Jg1"/11(J(Jrfr
- Page 74 and 75:
IonsFig. 74 Histological pictures s
- Page 76 and 77:
IonseM' Selecfofherm equipment-_s1S
- Page 78 and 79:
.....-------................',..,-n
- Page 80 and 81:
eM/rot gro"/!.Histologicallyconfirm
- Page 82 and 83:
A1er tnit,almonipulotionsand III«l
- Page 84 and 85:
Q'CSlNltftning1A. QfQ/-fJlf1inguQ
- Page 86 and 87:
otllm'lv.2 h th ju tifi d pro p ct
- Page 88 and 89:
t48xlD J WsEhmmahooofMe ~crdieal, c
- Page 90 and 91:
old°z-/ImitMW mode of calcu/aflonC
- Page 92 and 93:
he cylindr'cal area upplied by the'
- Page 94 and 95:
Tn-T-~-----1~--~--~JaluralttJtranSi
- Page 96 and 97:
aPI)Ii:lcati?n with a patially very
- Page 98 and 99:
are triggered. At the same site, ho
- Page 100 and 101:
n respired again, the drop in respi
- Page 102 and 103:
Exholationtubeloop aroundcmebroncll
- Page 104 and 105:
[Xeftt of,t"". Respiratorv... stand
- Page 106 and 107:
ventieFig. 112 pH decrease between
- Page 108 and 109:
BIncorporation ofJ5s-slI"ate intofh
- Page 110 and 111:
~LFig. 115 Electron micrograph of h
- Page 112 and 113:
12111098V ~ .-"~"' .....b""", ".1Tt
- Page 114 and 115:
,,,;tt cola;, ofH1e 88JIJitKIJIIl "
- Page 116 and 117:
"-1r-180 I'\112007(J)Jr' '- jwry¥I