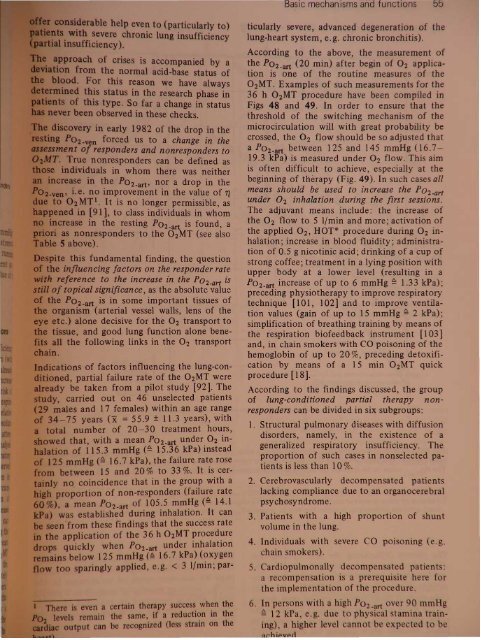
logical foundations13IrPtz12.........- ....... ~ .,f-IJ960 8o 2 4 614 16 188 KJ 12It ..Fig.47 Example of the behavior of the arterial resting P02 during the 02MT treatment of real nonresponders(slowing of respiration by 02 excess). Mean values of 3 patients [92]lOllThe main indication for the 02MT proceduresshould be seen as the prevention of illness.These procedures should always be used forprophylaxis at certain time intervals derivedfrom P02 measurements, in cases of pathologicalmovement disability or after approximatelythe 55th year of life (even earlier in exceptionalcases of levels P0 2 _ art < 70 mmHg Q9.3 kPa). In youth and middle age daily strenousexercise training (leisure sport, jogging, runningetc.) [12, 88, 95] is generally sufficient as ameans of permanently increasing the value of fl,or the Po 2 - art .1.1.8.6 Lung-conditioned, 02MT partial nonresponden; influencing facton, contra-indicationsLike every other therapeutic procedure, the02MT also has contraindications and therapynonresponders. There is usually a contraindicationfor patients in whom the body's respiratoryregulation is not controlled as normal bythe PC02 of the blood, but primarily by thelow P0 2of the blood (Loeschke's effect [96,97]). In these patients the 02MT can only beperformed with special precautions·.In some patients, as Fig. 47 shows, even a reductionin the arterial resting P0 2 of roughly5 mmHg due to the 02MT procedure was observed.In these patients a drop in the P02- venunder 02MT must have been attained.As is known [96, 97], the arterial hypoxemiawhich exists in generalized respiratory insufficiencyis associated with an 02 deficient controlof ventilation. Application of O2 eliminates• Artificial respiration if necessary. Recognition ofparen with abnormal respiration regulation bymeans of initial test, e.g. with checking of the bloode. or the dangers of artificial respiration for patienwith severe chronic respiratory insufficiency02 air mixtures with 02 proportions> 50%(JellPUatory depre ion, arterial P 02 60 mmHg,the adequate stimulus for the 02 deficiencyreceptor, and so alveolar hypoventilation (withthe reduction in the resting P02-8rt alreadymentioned), and also, in such cases, in increasein the PC02_art (hypercapnia) and the risk ofapnea can occur. When the generalized respiratoryinsufficiency is considered to be a relativecontraindication [98, 99], which is absoluteunder outpatient conditions, and when attentionis carefully paid to the blood gas analysisand the acid-base balance in partial respiratoryinsufficiency, where we have never observedany dysfunctions, the 02MT has proven iprincipal applicability under these circumstances,too. The temporary inhalation of.oxygen in patients with chronic lung di aand consecutive cor pulmonale has been ucessfully practised with the aim of redu ingresistance in the lesser circulation for[100]. Whether, and to what e tent, thcould have a comparable If ct i to bsubject of future inve tigation ppropriin pulmologically ori nt d tr atm nt nHowever, there can hardly b any ri f rpati nt in our th rapy progr m . hdoubling or trebling of th O 2 ont n iinhalation air in th 6 h pr do MT, or th t chnology d v 1 d f r ·
Ip even to (particularly to)severe chronic lung insufficiencylDffi,cien1ey).c .ses is accompanied by ahe normal acid-base status ofthis reason we have alwaystatus in the research phase inype. So far a change in statusobserved in these checks.eV6lrY In early 1982 of the drop in the-"Jft forced us to a change in the01 responders and nonresponders toe nonresponders can be defined astjjldi~ri'duals in whom there was neithere in the P02-art, nor a drop in thee. no improvement in the value of 112MTI. It is no longer permissible, asIn [91], to class individuals in whome in the resting P02- art is found, anonresponders to the 02MT (see alsoabove).this fundamental finding, the questionmfluencing factors on the responder rateterence to the increase in. the P0 2 -art istopical significance, as the absolute valueP02-art is in some important tissues ofmpnism (arterial vessel walls, lens of thec.) alone decisive for the O2 transport toe, and good lung function alone benethefollowing links in the O2 transporttions of factors influencing the lung-coned,partial failure rate of the 02MT werey be taken from a pilot study [92]. Thecarried out on 46 unselected patients,ales and 17 females) within an age range-75 years (x = 55.9 ± 11.3 years), withnumber of 20-30 treatment hours,d that, with a mean P0 2 - art under O2 inof115.3 mmHg (~ 15.36 kPa) insteadmHg (~ 16.7 kPa), the failure rate rosebe ween 15 and 20% to 33 %. It is cerno.coincidence that in the gro~p with aoportion of non-responders (fallure ratea mean P02-art of 105.5 mmHg (~ 14.1a established during inhalation. It cann from these findings that the success rateapplication of the 36 h 02MT procedurequickly when P0 2 - art under inhalationbelow 125 mmHg (~ 16.7 kPa) (oxygenparingly applied, e.g. < 3 I/min; parevena certain therapy success when themain the arne, if a reduction in theoutput can be recognized (less train on theticularly severe, advanced degeneration of thelung-heart system, e.g. chronic bronchitis).According to the above, the measurement ofthe P02- art (20 min) after begin of O 2 applicationis one of the routine measures of the02MT. Examples of such measurements for the36 h 02MT procedure have been compiled inFigs 48 and 49. In order to ensure that thethreshold of the switching mechanism of themicrocirculation will with great probability becrossed, the O2 flow should be so adjusted thata P02- art between 125 and 145 mmHg (16.719.3 kPa) is measured under O2 flow. This aimis often difficult to achieve, especially at thebeginning of therapy (Fig. 49). In such cases allmeans should be used to increase the P0 2 -artunder O 2 inhalation during the first sessions.The adjuvant means include: the increase ofthe O2 flow to 5 Ilmin and more; activation ofthe applied O2, HOT* procedure during 02 inhalation;increase in blood fluidity; administrationof 0.5 g nicotinic acid; drinking of a cup ofstrong coffee; treatment in a lying position withupper body at a lower level (resulting in aP02-art increase of up to 6 mmHg ~ 1.33 kPa);preceding physiotherapy to improve respiratorytechnique [101, 102] and to improve ventilationvalues (gain of up to 15 mmHg ~ 2 kPa);simplification of breathing training by means ofthe respiration biofeedback instrument [103]and, in chain smokers with CO poisoning of thehemoglobin of up to 20 %, preceding detoxificationby means of a 15 min 02MT quickprocedure [18].According to the findings discussed, the groupof lung-conditioned partial therapy nonresponderscan be divided in six subgroups:1. Structural pulmonary diseases with diffusiondisorders, namely, in the existence of ageneralized respiratory insufficiency. Theproportion of such cases in nonselected patientsis less than 10 %.2. Cerebrovascularly decompensated patientslacking compliance due to an organocerebralpsychosyndrome.3. Patients with a high proportion of huntvolume in the lung.4. Individuals with severe CO poi oning ( .g.chain smokers).5. Cardiopulmonally decomp n at d p ti nt :a recompensation i a pr r qui it h f rthe implem ntation of th pr dur.6. In per on with a high P0 2 -art r 0 mm~ 12 kPa .g. du t ph i 1 t min r ining),a high r I v I annot b t t
- Page 1 and 2: sand functl ni ove d cellular capil
- Page 3: 8 1. Physiological fou~dationsmmHga
- Page 6 and 7: Basic mechanisms and functions 11e
- Page 8 and 9: Basic mechanisms and functions 13pr
- Page 11 and 12: 500r-T_-+5__r-_-+1O__,....-_~15.1O-
- Page 13 and 14: ~IUI1!J ~atpWorMs---~~·tIIlDkeJ \I
- Page 15 and 16: y r na onabS,olu'te clla.ra~t ri ti
- Page 17 and 18: 100907065"I 4y iological foundation
- Page 19 and 20: 1. hy lologlcal foundations70"''''J
- Page 21 and 22: CII'Cli8LC outl)ut VAr;lllil i e re
- Page 23 and 24: -'0 y 101091cai oundatlons80%6050l~
- Page 25 and 26: ,..._........,.--~"'!""!!'!~~----_.
- Page 27 and 28: hi v d in h arrangement shown above
- Page 29 and 30: 34 1. Physiological foundations70%6
- Page 31 and 32: logical foundationsu .on in the opt
- Page 33 and 34: 1. Physiological foundations. ~ la~
- Page 35 and 36: II foundationsI tem IBPtrsons with
- Page 37: 1. Physiological foundationsAirdosi
- Page 40 and 41: 110N.ttJJOt~1. Physiological founda
- Page 42 and 43: 1. Phy iological foundationsAnoO;HT
- Page 44 and 45: hysiological foundations...fJJHT(JI
- Page 46 and 47: 1. Physiological foundationsCOCOM I
- Page 48 and 49: g r d, whi h con iderably contribut
- Page 52 and 53: ,. Physiological foundationsIf-RoN
- Page 54 and 55: 1. Physiological foundationsAll"i1t
- Page 56 and 57: ~~itItINitIIJq/s N 31 54 52~IBIP~-.
- Page 58 and 59: BDuring OzMTprocedurecAfter OzMTpro
- Page 60 and 61: A Bi3lrfss 1'1oafofmovement 8 0pl'r
- Page 62 and 63: Table 6 PO b measurements of unsele
- Page 64 and 65: serert~ hyperoxia pure 0 } .distres
- Page 66 and 67: IIstress qirI/iII mn wryhJI1IJSISLo
- Page 68 and 69: A/JtfJtnk«P~1Mtrr'ttriIWIItJfIS~.~
- Page 70 and 71: Table 7 The change in the architect
- Page 72 and 73: nsMslor rotd'1uI.-Jl!Jg1"/11(J(Jrfr
- Page 74 and 75: IonsFig. 74 Histological pictures s
- Page 76 and 77: IonseM' Selecfofherm equipment-_s1S
- Page 78 and 79: .....-------................',..,-n
- Page 80 and 81: eM/rot gro"/!.Histologicallyconfirm
- Page 82 and 83: A1er tnit,almonipulotionsand III«l
- Page 84 and 85: Q'CSlNltftning1A. QfQ/-fJlf1inguQ
- Page 86 and 87: otllm'lv.2 h th ju tifi d pro p ct
- Page 88 and 89: t48xlD J WsEhmmahooofMe ~crdieal, c
- Page 90 and 91: old°z-/ImitMW mode of calcu/aflonC
- Page 92 and 93: he cylindr'cal area upplied by the'
- Page 94 and 95: Tn-T-~-----1~--~--~JaluralttJtranSi
- Page 96 and 97: aPI)Ii:lcati?n with a patially very
- Page 98 and 99: are triggered. At the same site, ho
- Page 100 and 101:
n respired again, the drop in respi
- Page 102 and 103:
Exholationtubeloop aroundcmebroncll
- Page 104 and 105:
[Xeftt of,t"". Respiratorv... stand
- Page 106 and 107:
ventieFig. 112 pH decrease between
- Page 108 and 109:
BIncorporation ofJ5s-slI"ate intofh
- Page 110 and 111:
~LFig. 115 Electron micrograph of h
- Page 112 and 113:
12111098V ~ .-"~"' .....b""", ".1Tt
- Page 114 and 115:
,,,;tt cola;, ofH1e 88JIJitKIJIIl "
- Page 116 and 117:
"-1r-180 I'\112007(J)Jr' '- jwry¥I