

Thursday-Abstracts
Thursday-Abstracts
Thursday-Abstracts

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Thursday</strong>, May 30, 2013<br />
S190 Vol. 45 No. 5 Supplement<br />
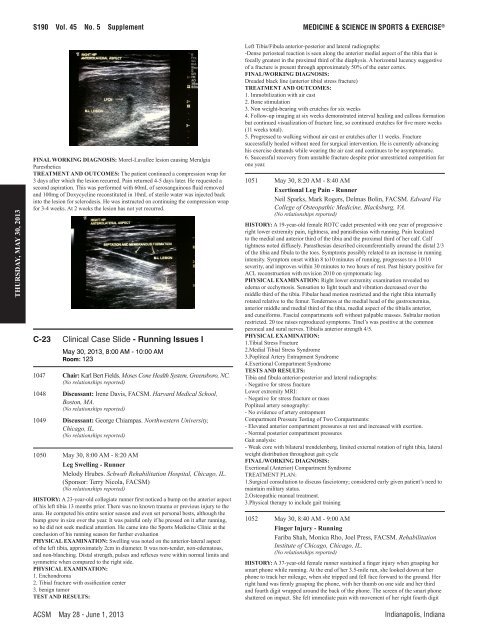
FINaL WOrKING dIaGNOsIs: Morel-Lavallee lesion causing Meralgia<br />
Paresthetica<br />
TrEaTMENT aNd OuTCOMEs: The patient continued a compression wrap for<br />
3 days after which the lesion recurred. Pain returned 4-5 days later. He requested a<br />
second aspiration. This was performed with 60mL of serosanguinous fluid removed<br />
and 100mg of Doxycycline reconstituted in 10mL of sterile water was injected back<br />
into the lesion for sclerodesis. He was instructed on continuing the compression wrap<br />
for 3-4 weeks. At 2 weeks the lesion has not yet recurred.<br />
C-23 Clinical Case Slide - Running Issues I<br />
May 30, 2013, 8:00 AM - 10:00 AM<br />
Room: 123<br />
1047 Chair: Karl Bert Fields. Moses Cone Health System, Greensboro, NC.<br />
(No relationships reported)<br />
1048 discussant: Irene Davis, FACSM. Harvard Medical School,<br />
Boston, MA.<br />
(No relationships reported)<br />
1049 discussant: George Chiampas. Northwestern University,<br />
Chicago, IL.<br />
(No relationships reported)<br />
1050 May 30, 8:00 AM - 8:20 AM<br />
Leg swelling - runner<br />
Melody Hrubes. Schwab Rehabilitation Hospital, Chicago, IL.<br />
(Sponsor: Terry Nicola, FACSM)<br />
(No relationships reported)<br />
hIsTOry: A 23-year-old collegiate runner first noticed a bump on the anterior aspect<br />
of his left tibia 13 months prior. There was no known trauma or previous injury to the<br />
area. He competed his entire senior season and even set personal bests, although the<br />
bump grew in size over the year. It was painful only if he pressed on it after running,<br />
so he did not seek medical attention. He came into the Sports Medicine Clinic at the<br />
conclusion of his running season for further evaluation<br />
PhysICaL EXaMINaTION: Swelling was noted on the anterior-lateral aspect<br />
of the left tibia, approximately 2cm in diameter. It was non-tender, non-edematous,<br />
and non-blanching. Distal strength, pulses and reflexes were within normal limits and<br />
symmetric when compared to the right side.<br />
PhysICaL EXaMINaTION:<br />
1. Enchondroma<br />
2. Tibial fracture with ossification center<br />
3. benign tumor<br />
TEsT aNd rEsuLTs:<br />
MEDICINE & SCIENCE IN SPORTS & EXERCISE ®<br />
Left Tibia/Fibula anterior-posterior and lateral radiographs:<br />
-Dense periosteal reaction is seen along the anterior medial aspect of the tibia that is<br />
focally greatest in the proximal third of the diaphysis. A horizontal lucency suggestive<br />
of a fracture is present through approximately 50% of the outer cortex.<br />
FINaL/WOrKING dIaGNOsIs:<br />
Dreaded black line (anterior tibial stress fracture)<br />
TrEaTMENT aNd OuTCOMEs:<br />
1. Immobilization with air cast<br />
2. Bone stimulation<br />
3. Non weight-bearing with crutches for six weeks<br />
4. Follow-up imaging at six weeks demonstrated interval healing and callous formation<br />
but continued visualization of fracture line, so continued crutches for five more weeks<br />
(11 weeks total).<br />
5. Progressed to walking without air cast or crutches after 11 weeks. Fracture<br />
successfully healed without need for surgical intervention. He is currently advancing<br />
his exercise demands while wearing the air cast and continues to be asymptomatic.<br />
6. Successful recovery from unstable fracture despite prior unrestricted competition for<br />
one year.<br />
1051 May 30, 8:20 AM - 8:40 AM<br />
Exertional Leg Pain - runner<br />
Neil Sparks, Mark Rogers, Delmas Bolin, FACSM. Edward Via<br />
College of Osteopathic Medicine, Blacksburg, VA.<br />
(No relationships reported)<br />
hIsTOry: A 19-year-old female ROTC cadet presented with one year of progressive<br />
right lower extremity pain, tightness, and parasthesias with running. Pain localized<br />
to the medial and anterior third of the tibia and the proximal third of her calf. Calf<br />
tightness noted diffusely. Parasthesias described circumferentially around the distal 2/3<br />
of the tibia and fibula to the toes. Symptoms possibly related to an increase in running<br />
intensity. Symptom onset within 8 to10 minutes of running, progresses to a 10/10<br />
severity, and improves within 30 minutes to two hours of rest. Past history positive for<br />
ACL reconstruction with revision 2010 on symptomatic leg.<br />
PhysICaL EXaMINaTION: Right lower extremity examination revealed no<br />
edema or ecchymosis. Sensation to light touch and vibration decreased over the<br />
middle third of the tibia. Fibular head motion restricted and the right tibia internally<br />
rotated relative to the femur. Tenderness at the medial head of the gastrocnemius,<br />
anterior middle and medial third of the tibia, medial aspect of the tibialis anterior,<br />
and cuneiforms. Fascial compartments soft without palpable masses. Subtalar motion<br />
restricted. 20 toe raises reproduced symptoms. Tinel’s was positive at the common<br />
peroneal and sural nerves. Tibialis anterior strength 4/5.<br />
PhysICaL EXaMINaTION:<br />
1.Tibial Stress Fracture<br />
2.Medial Tibial Stress Syndrome<br />
3.Popliteal Artery Entrapment Syndrome<br />
4.Exertional Compartment Syndrome<br />
TEsTs aNd rEsuLTs:<br />
Tibia and fibula anterior-posterior and lateral radiographs:<br />
- Negative for stress fracture<br />
Lower extremity MRI:<br />
- Negative for stress fracture or mass<br />
Popliteal artery sonography:<br />
- No evidence of artery entrapment<br />
Compartment Pressure Testing of Two Compartments:<br />
- Elevated anterior compartment pressures at rest and increased with exertion.<br />
- Normal posterior compartment pressures<br />
Gait analysis:<br />
- Weak core with bilateral trendelenberg, limited external rotation of right tibia, lateral<br />
weight distribution throughout gait cycle<br />
FINaL/WOrKING dIaGNOsIs:<br />
Exertional (Anterior) Compartment Syndrome<br />
TREATMENT PLAN:<br />
1.Surgical consultation to discuss fasciotomy; considered early given patient’s need to<br />
maintain military status.<br />
2.Osteopathic manual treatment.<br />
3.Physical therapy to include gait training<br />
1052 May 30, 8:40 AM - 9:00 AM<br />
Finger Injury - running<br />
Fariba Shah, Monica Rho, Joel Press, FACSM. Rehabilitation<br />
Institute of Chicago, Chicago, IL.<br />
(No relationships reported)<br />
hIsTOry: A 37-year-old female runner sustained a finger injury when grasping her<br />
smart phone while running. At the end of her 3.5-mile run, she looked down at her<br />
phone to track her mileage, when she tripped and fell face forward to the ground. Her<br />
right hand was firmly grasping the phone, with her thumb on one side and her third<br />
and fourth digit wrapped around the back of the phone. The screen of the smart phone<br />
shattered on impact. She felt immediate pain with movement of her right fourth digit<br />
ACSM May 28 - June 1, 2013 Indianapolis, Indiana