Radiography in Modern Industry - Kodak
Radiography in Modern Industry - Kodak
Radiography in Modern Industry - Kodak

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
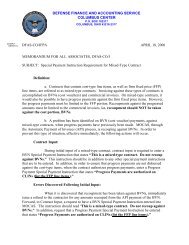
Figure 98: Characteristic curve of a typical film used for duplicat<strong>in</strong>g radiographs.Further, the gradients of the duplicat<strong>in</strong>g films are -1.0 over their useful density range. This meansthat, with<strong>in</strong> this range, density differences <strong>in</strong> the orig<strong>in</strong>al radiograph are faithfully reproduced <strong>in</strong>the copy.ExposureThe exposure technique for duplicat<strong>in</strong>g film is simple and may be varied to suit the equipmentavailable. The radiograph to be copied is put <strong>in</strong> a glass-fronted pr<strong>in</strong>t<strong>in</strong>g frame (available fromdealers <strong>in</strong> photographic supplies). A sheet of duplicat<strong>in</strong>g film is placed on top of the radiograph,emulsion side <strong>in</strong> contact with the radiograph to be copied. The back of the pr<strong>in</strong>t<strong>in</strong>g frame is closedand an exposure to light is made through the glass. Any convenient light source can be used, andthus exposure conditions are difficult to specify. However, a conventional fluorescent x-rayillum<strong>in</strong>ator is a usable light source. At a distance of about 2 feet between illum<strong>in</strong>ator and pr<strong>in</strong>t<strong>in</strong>gframe, exposures range from several seconds to a m<strong>in</strong>ute. These exposures are long enough totime conveniently with simple means yet short enough to be efficient.When a satisfactory exposure time has been found by trial for a particular radiograph, exposuresfor others can be estimated much more accurately. The densities <strong>in</strong> the areas of <strong>in</strong>terest of thetwo radiographs are read, and subtracted one from the other. The antilogarithm of this densitydifference is the factor by which the orig<strong>in</strong>al exposure must be multiplied (if the secondradiograph is darker than the first) or divided (if the second radiograph is the lighter).Care should be taken to keep the glass front of the pr<strong>in</strong>t<strong>in</strong>g frame free from dirt, because anyth<strong>in</strong>gopaque adher<strong>in</strong>g to the glass appears as a dark mark on the processed duplicate.Reproduction of DensitiesAs shown by the characteristic curve of Figure 98, the maximum density obta<strong>in</strong>able (that is, withno exposure on the duplicat<strong>in</strong>g film) may be below the maximum density <strong>in</strong> the radiograph to becopied. Thus, if the densities <strong>in</strong> the areas of <strong>in</strong>terest <strong>in</strong> an <strong>in</strong>dustrial radiograph were 3.0 and 3.5,the duplicat<strong>in</strong>g film, the curve of which is shown <strong>in</strong> Figure 98, could not reproduce thesedensities. It would, however, reproduce the density differences exactly, and thus reproduceexactly the radiographic contrasts of the orig<strong>in</strong>al. If the densities <strong>in</strong> the orig<strong>in</strong>al were 3.0 and 3.5,these could be reproduced as 0.7 and 1.2, respectively or 1.0 and 1.5, or 1.3 and 1.8, depend<strong>in</strong>gon the exposure given the duplicat<strong>in</strong>g film.In many cases, a reproduction of the radiographic contrasts alone is quite sufficient. (Note that ifa radiograph with densities of 1.0 and 1.5 were displayed on an illum<strong>in</strong>ator, and a similarradiograph but with densities of 3.0 and 3.5 were displayed on an illum<strong>in</strong>ator 100 times as bright,an observer would be unable to dist<strong>in</strong>guish between them.)<strong>Radiography</strong> <strong>in</strong> <strong>Modern</strong> <strong>Industry</strong> 160