

Is headspace making a difference to young people’s lives?
Evaluation-of-headspace-program
Evaluation-of-headspace-program

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
5. Service Delivery Model<br />
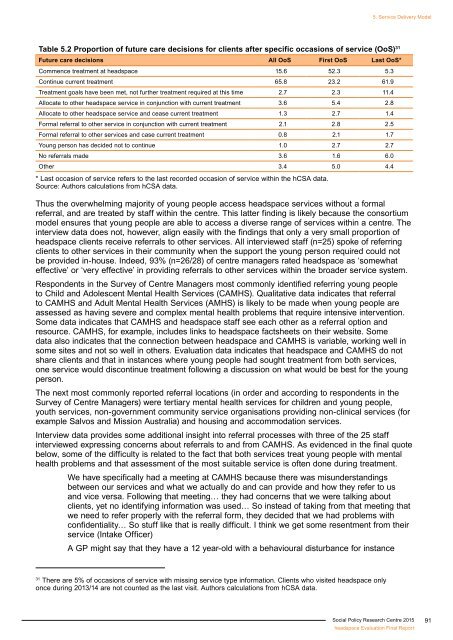
Table 5.2 Proportion of future care decisions for clients after specific occasions of service (OoS) 31<br />
Future care decisions All OoS First OoS Last OoS*<br />
Commence treatment at <strong>headspace</strong> 15.6 52.3 5.3<br />
Continue current treatment 65.8 23.2 61.9<br />
Treatment goals have been met, not further treatment required at this time 2.7 2.3 11.4<br />
Allocate <strong>to</strong> other <strong>headspace</strong> service in conjunction with current treatment 3.6 5.4 2.8<br />
Allocate <strong>to</strong> other <strong>headspace</strong> service and cease current treatment 1.3 2.7 1.4<br />
Formal referral <strong>to</strong> other service in conjunction with current treatment 2.1 2.8 2.5<br />
Formal referral <strong>to</strong> other services and case current treatment 0.8 2.1 1.7<br />
Young person has decided not <strong>to</strong> continue 1.0 2.7 2.7<br />
No referrals made 3.6 1.6 6.0<br />
Other 3.4 5.0 4.4<br />
* Last occasion of service refers <strong>to</strong> the last recorded occasion of service within the hCSA data.<br />
Source: Authors calculations from hCSA data.<br />
Thus the overwhelming majority of <strong>young</strong> people access <strong>headspace</strong> services without a formal<br />
referral, and are treated by staff within the centre. This latter finding is likely because the consortium<br />
model ensures that <strong>young</strong> people are able <strong>to</strong> access a diverse range of services within a centre. The<br />
interview data does not, however, align easily with the findings that only a very small proportion of<br />
<strong>headspace</strong> clients receive referrals <strong>to</strong> other services. All interviewed staff (n=25) spoke of referring<br />
clients <strong>to</strong> other services in their community when the support the <strong>young</strong> person required could not<br />
be provided in-house. Indeed, 93% (n=26/28) of centre managers rated <strong>headspace</strong> as ‘somewhat<br />
effective’ or ‘very effective’ in providing referrals <strong>to</strong> other services within the broader service system.<br />
Respondents in the Survey of Centre Managers most commonly identified referring <strong>young</strong> people<br />
<strong>to</strong> Child and Adolescent Mental Health Services (CAMHS). Qualitative data indicates that referral<br />
<strong>to</strong> CAMHS and Adult Mental Health Services (AMHS) is likely <strong>to</strong> be made when <strong>young</strong> people are<br />
assessed as having severe and complex mental health problems that require intensive intervention.<br />
Some data indicates that CAMHS and <strong>headspace</strong> staff see each other as a referral option and<br />
resource. CAMHS, for example, includes links <strong>to</strong> <strong>headspace</strong> factsheets on their website. Some<br />
data also indicates that the connection between <strong>headspace</strong> and CAMHS is variable, working well in<br />
some sites and not so well in others. Evaluation data indicates that <strong>headspace</strong> and CAMHS do not<br />
share clients and that in instances where <strong>young</strong> people had sought treatment from both services,<br />
one service would discontinue treatment following a discussion on what would be best for the <strong>young</strong><br />
person.<br />
The next most commonly reported referral locations (in order and according <strong>to</strong> respondents in the<br />
Survey of Centre Managers) were tertiary mental health services for children and <strong>young</strong> people,<br />
youth services, non-government community service organisations providing non-clinical services (for<br />
example Salvos and Mission Australia) and housing and accommodation services.<br />
Interview data provides some additional insight in<strong>to</strong> referral processes with three of the 25 staff<br />
interviewed expressing concerns about referrals <strong>to</strong> and from CAMHS. As evidenced in the final quote<br />
below, some of the difficulty is related <strong>to</strong> the fact that both services treat <strong>young</strong> people with mental<br />
health problems and that assessment of the most suitable service is often done during treatment.<br />
We have specifically had a meeting at CAMHS because there was misunderstandings<br />
between our services and what we actually do and can provide and how they refer <strong>to</strong> us<br />
and vice versa. Following that meeting… they had concerns that we were talking about<br />
clients, yet no identifying information was used… So instead of taking from that meeting that<br />
we need <strong>to</strong> refer properly with the referral form, they decided that we had problems with<br />
confidentiality… So stuff like that is really difficult. I think we get some resentment from their<br />
service (Intake Officer)<br />
A GP might say that they have a 12 year-old with a behavioural disturbance for instance<br />
31<br />
There are 5% of occasions of service with missing service type information. Clients who visited <strong>headspace</strong> only<br />
once during 2013/14 are not counted as the last visit. Authors calculations from hCSA data.<br />
Social Policy Research Centre 2015<br />
<strong>headspace</strong> Evaluation Final Report<br />
91