

vol21no7_pdf-version
vol21no7_pdf-version
vol21no7_pdf-version

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
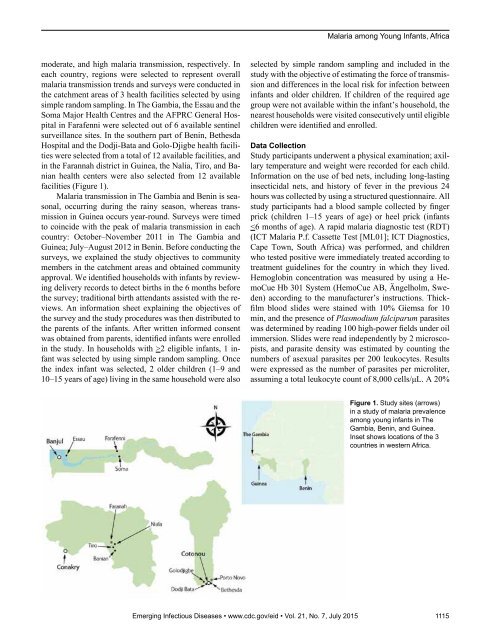
Malaria among Young Infants, Africamoderate, and high malaria transmission, respectively. Ineach country, regions were selected to represent overallmalaria transmission trends and surveys were conducted inthe catchment areas of 3 health facilities selected by usingsimple random sampling. In The Gambia, the Essau and theSoma Major Health Centres and the AFPRC General Hospitalin Farafenni were selected out of 6 available sentinelsurveillance sites. In the southern part of Benin, BethesdaHospital and the Dodji-Bata and Golo-Djigbe health facilitieswere selected from a total of 12 available facilities, andin the Farannah district in Guinea, the Nalia, Tiro, and Banianhealth centers were also selected from 12 availablefacilities (Figure 1).Malaria transmission in The Gambia and Benin is seasonal,occurring during the rainy season, whereas transmissionin Guinea occurs year-round. Surveys were timedto coincide with the peak of malaria transmission in eachcountry: October–November 2011 in The Gambia andGuinea; July–August 2012 in Benin. Before conducting thesurveys, we explained the study objectives to communitymembers in the catchment areas and obtained communityapproval. We identified households with infants by reviewingdelivery records to detect births in the 6 months beforethe survey; traditional birth attendants assisted with the reviews.An information sheet explaining the objectives ofthe survey and the study procedures was then distributed tothe parents of the infants. After written informed consentwas obtained from parents, identified infants were enrolledin the study. In households with >2 eligible infants, 1 infantwas selected by using simple random sampling. Oncethe index infant was selected, 2 older children (1–9 and10–15 years of age) living in the same household were alsoselected by simple random sampling and included in thestudy with the objective of estimating the force of transmissionand differences in the local risk for infection betweeninfants and older children. If children of the required agegroup were not available within the infant’s household, thenearest households were visited consecutively until eligiblechildren were identified and enrolled.Data CollectionStudy participants underwent a physical examination; axillarytemperature and weight were recorded for each child.Information on the use of bed nets, including long-lastinginsecticidal nets, and history of fever in the previous 24hours was collected by using a structured questionnaire. Allstudy participants had a blood sample collected by fingerprick (children 1–15 years of age) or heel prick (infants