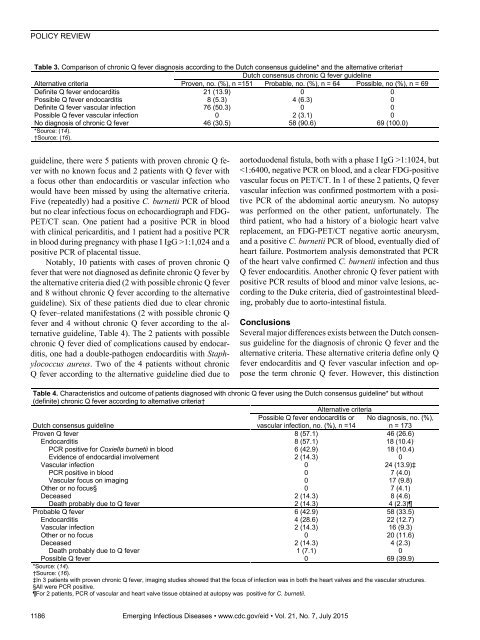
POLICY REVIEWTable 3. Comparison of chronic Q fever diagnosis according to the Dutch consensus guideline* and the alternative criteria†Dutch consensus chronic Q fever guidelineAlternative criteriaProven, no. (%), n =151 Probable, no. (%), n = 64 Possible, no (%), n = 69Definite Q fever endocarditis 21 (13.9) 0 0Possible Q fever endocarditis 8 (5.3) 4 (6.3) 0Definite Q fever vascular infection 76 (50.3) 0 0Possible Q fever vascular infection 0 2 (3.1) 0No diagnosis of chronic Q fever 46 (30.5) 58 (90.6) 69 (100.0)*Source: (14).†Source: (16).guideline, there were 5 patients with proven chronic Q feverwith no known focus and 2 patients with Q fever witha focus other than endocarditis or vascular infection whowould have been missed by using the alternative criteria.Five (repeatedly) had a positive C. burnetii PCR of bloodbut no clear infectious focus on echocardiograph and FDG-PET/CT scan. One patient had a positive PCR in bloodwith clinical pericarditis, and 1 patient had a positive PCRin blood during pregnancy with phase I IgG >1:1,024 and apositive PCR of placental tissue.Notably, 10 patients with cases of proven chronic Qfever that were not diagnosed as definite chronic Q fever bythe alternative criteria died (2 with possible chronic Q feverand 8 without chronic Q fever according to the alternativeguideline). Six of these patients died due to clear chronicQ fever–related manifestations (2 with possible chronic Qfever and 4 without chronic Q fever according to the alternativeguideline, Table 4). The 2 patients with possiblechronic Q fever died of complications caused by endocarditis,one had a double-pathogen endocarditis with Staphylococcusaureus. Two of the 4 patients without chronicQ fever according to the alternative guideline died due toaortoduodenal fistula, both with a phase I IgG >1:1024, but
Chronic Q Fever Diagnosisis not accompanied by therapeutic consequences for eachof these manifestations, which we believe makes theseguidelines less practical.It must be acknowledged that, because all patients includedin our study met the Dutch criteria for proven, probable,or possible chronic Q fever, other guidelines can onlyperform with less accuracy in comparison. Nevertheless,sensitivity of the Dutch guideline is markedly higher thanwith the alternative criteria: ≈31% of proven chronic Q fevercase-patients would have been missed as well as almostall patients with probable and possible cases, including atleast 4 patients who eventually died of chronic Q fever relatedcauses. Specificity of the Dutch consensus guidelineis probably lower than that of the alternative criteria, butbecause mortality and morbidity rates are high when chronicQ fever cases are untreated, we believe sensitivity is ofgreater importance in clinical practice. Our data illustratethat, when proven cases of chronic Q fever are missed, andpatients are therefore not adequately treated, these patientsare at high risk for severe complications and death.As stated before, the most critical difference betweenthe criteria of the Dutch guideline and those of the alternativeguideline is the acknowledgment of a positive C. burnetiiPCR as a marker of proven chronic Q fever in the absenceof acute Q fever. Of course, this difference should beinterpreted with care. In our opinion, patients without endocarditisor vascular infection on imaging studies but witha positive PCR in blood should also be treated for chronicQ fever, as they may suffer from not yet clinically visibleendocarditis or vascular infection, which was confirmed bythe postmortem results of 2 of our patients described above.A single positive C. burnetii PCR of blood is highly suggestivefor chronic Q fever when acute Q fever is excluded.A PCR test will not be performed in patients without symptomsand without any risk factors for chronic Q fever, socases in whom a positive PCR is the only factor indicatingchronic Q fever is a theoretical consideration. We haveobserved few patients, in the absence of signs of acute Qfever, with elevated phase I IgG titers not fulfilling the serologiccriteria of chronic Q fever (phase I IgG ≥1:800 or1,024) but with a positive C. burnetii PCR of blood or tissue.In these cases, we are convinced that PCR-positivityproves chronic Q fever. No patients in our chronic Q feverdatabase who had a positive PCR on blood or tissue had aphase I IgG titer of ≤1:256.We agree with the statement that proven chronic Q feverwill not develop in some patients with probable chronicQ fever and in most patients with possible chronic Q fever.We therefore do not advocate treating all of these patientswith long-term antibacterial drugs. Nevertheless, wedo think that these patients should all be examined for achronic Q fever focus and should continue to be monitoredclosely, at least until further research offers more clarityregarding the prognosis of these patients. If these patientsdo not receive a diagnosis of possible or probable chronic Qfever, they might not receive such close follow-up. Moreover,the Dutch consensus guideline is easier to use, addstreatment advice, and also applies to patients with chronicQ fever manifestations that are rarer than endocarditis andvascular infection.We hope that, with the future results from the DutchNational Chronic Q Fever Database and joint efforts ofinternational researchers and experts in the field of Q fever,these guidelines can be modified to provide definiteevidence-based criteria for diagnosis and treatment of thiscomplex disease. In the meantime, the Dutch consensusguideline created on the basis of the scarce available literatureis, in our opinion, safer and easier to use in clinicalpractice than the alternative expert-based criteria.AcknowledgmentsWe thank all participants in the Dutch National Chronic QFever Database in the Netherlands: Monique de Jager-Leclercq(Bernhoven Hospital, Oss), Cornelis A.R. Groot (BernhovenHospital), Yvonne Soethoudt (Elkerliek Hospital, Helmond),Sybrandus N. Blank (Maxima Medical Center, Eindhoven/Veldhoven),Marjolijn J.H. Pronk (Catharina Hospital, Eindhoven),Gijs J. Limonard (Diakonessenhuis, Utrecht), Steven F. Thijssen(Diakonessenhuis), Bart J. Vlaminckx (St Antonius Hospital,Nieuwegein), Jacqueline Buijs (Atrium Medical Center, Heerlen),Bas J.M van Kraaij (Atrium Medical Center), FrederikaDijkstra (Centre for Infectious Disease Control, Bilthoven),Clemens Richter (Rijnstate Hospital, Arnhem), E.H. Gisolf (RijnstateHospital, Arnhem), Rik Heijligenberg (Gelderse ValleiHospital, Ede), Ries Schouten (Gelderse Vallei Hospital), KarinSchurink (Erasmus University Medical Center, Rotterdam), LeoG. Visser (Leiden University Medical Center, Leiden).Dr. Kampschreur is a physician and PhD researcher in the Divisionof Medicine, Department of Internal Medicine and InfectiousDiseases, University Medical Center Utrecht. Her recent researchfocuses on chronic Q fever in the Netherlands.References1. Maurin M, Raoult D. Q fever. Clin Microbiol Rev. 1999;12:518–53.2. van der Hoek W, Dijkstra F, Schimmer B, Schneeberger PM,Vellema P, Wijkmans C, et al. Q fever in the Netherlands: anupdate on the epidemiology and control measures. Euro Surveill.2010;15:19520.3. Delsing CE, Kullberg BJ, Bleeker-Rovers CP. Q fever in theNetherlands from 2007 to 2010. Neth J Med. 2010;68:382–7.4. Landais C, Fenollar F, Thuny F, Raoult D. From acute Q feverto endocarditis: serological follow-up strategy. Clin Infect Dis.2007;44:1337–40. http://dx.doi.org/10.1086/5154015. Raoult D, Tissot-Dupont H, Foucault C, Gouvernet J, Fournier PE,Bernit E, et al. Q fever 1985–1998. Clinical and epidemiologicfeatures of 1,383 infections. Medicine (Baltimore). 2000;79:109–23. http://dx.doi.org/10.1097/00005792-200003000-00005Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 21, No. 7, July 2015 1187
- Page 3 and 4:
July 2015SynopsisOn the CoverMarian
- Page 5 and 6:
1240 Gastroenteritis OutbreaksCause
- Page 7 and 8:
SYNOPSISDisseminated Infections wit
- Page 9 and 10:
Disseminated Infections with Talaro
- Page 11 and 12:
Disseminated Infections with Talaro
- Page 13 and 14:
Macacine Herpesvirus 1 inLong-Taile
- Page 15 and 16:
Macacine Herpesvirus 1 in Macaques,
- Page 17 and 18:
Macacine Herpesvirus 1 in Macaques,
- Page 19:
Macacine Herpesvirus 1 in Macaques,
- Page 23:
Malaria among Young Infants, Africa
- Page 26 and 27:
RESEARCHFigure 3. Dynamics of 19-kD
- Page 28 and 29:
Transdermal Diagnosis of MalariaUsi
- Page 30 and 31:
RESEARCHFigure 2. A) Acoustic trace
- Page 32 and 33:
RESEARCHof malaria-infected mosquit
- Page 34 and 35:
Lack of Transmission amongClose Con
- Page 36 and 37:
RESEARCH(IFA) and microneutralizati
- Page 38 and 39:
RESEARCHoropharyngeal, and serum sa
- Page 40 and 41:
RESEARCH6. Assiri A, McGeer A, Perl
- Page 42 and 43: RESEARCHadvanced genomic sequencing
- Page 44 and 45: RESEARCHTable 2. Next-generation se
- Page 46 and 47: RESEARCHTable 3. Mutation analysis
- Page 48 and 49: RESEARCHReferences1. Baize S, Panne
- Page 50 and 51: Parechovirus Genotype 3 Outbreakamo
- Page 52 and 53: RESEARCHFigure 1. Venn diagramshowi
- Page 54 and 55: RESEARCHTable 2. HPeV testing of sp
- Page 56 and 57: RESEARCHFigure 5. Distribution of h
- Page 58 and 59: RESEARCHReferences1. Selvarangan R,
- Page 60 and 61: RESEARCHthe left lobe was sampled b
- Page 62 and 63: RESEARCHTable 2. Middle East respir
- Page 64 and 65: RESEARCHseroprevalence in domestic
- Page 66 and 67: RESEARCHmeasure their current surve
- Page 68 and 69: RESEARCHTable 2. States with labora
- Page 70 and 71: RESEARCHFigure 2. Comparison of sur
- Page 72 and 73: RESEARCH9. Centers for Disease Cont
- Page 74 and 75: RESEARCHthe analyses. Cases in pers
- Page 76 and 77: RESEARCHTable 3. Sampling results (
- Page 78 and 79: RESEARCHpresence of Legionella spp.
- Page 80 and 81: Seroprevalence for Hepatitis Eand O
- Page 82 and 83: RESEARCHTable 1. Description of stu
- Page 84 and 85: RESEARCHTable 3. Crude and adjusted
- Page 86 and 87: RESEARCHrates by gender or HIV stat
- Page 88 and 89: RESEARCH25. Taha TE, Kumwenda N, Ka
- Page 90 and 91: POLICY REVIEWDutch Consensus Guidel
- Page 94 and 95: POLICY REVIEW6. Botelho-Nevers E, F
- Page 96 and 97: DISPATCHESFigure 1. Phylogenetic tr
- Page 98 and 99: DISPATCHESSevere Pediatric Adenovir
- Page 100 and 101: DISPATCHESTable 1. Demographics and
- Page 102 and 103: DISPATCHES13. Kim YJ, Hong JY, Lee
- Page 104 and 105: DISPATCHESTable. Alignment of resid
- Page 106 and 107: DISPATCHESFigure 2. Interaction of
- Page 108 and 109: DISPATCHESSchmallenberg Virus Recur
- Page 110 and 111: DISPATCHESFigure 2. Detection of Sc
- Page 112 and 113: DISPATCHESFigure 1. Histopathologic
- Page 114: DISPATCHESFigure 2. Detection of fo
- Page 117 and 118: Influenza Virus Strains in the Amer
- Page 119 and 120: Novel Arenavirus Isolates from Nama
- Page 121 and 122: Novel Arenaviruses, Southern Africa
- Page 123 and 124: Readability of Ebola Informationon
- Page 125 and 126: Readability of Ebola Information on
- Page 127 and 128: Patients under investigation for ME
- Page 129 and 130: Patients under investigation for ME
- Page 131 and 132: Wildlife Reservoir for Hepatitis E
- Page 133 and 134: Asymptomatic Malaria and Other Infe
- Page 135 and 136: Asymptomatic Malaria in Children fr
- Page 137 and 138: Bufavirus in Wild Shrews and Nonhum
- Page 139 and 140: Bufavirus in Wild Shrews and Nonhum
- Page 141 and 142: Range Expansion for Rat Lungworm in
- Page 143 and 144:
Slow Clearance of Plasmodium falcip
- Page 145 and 146:
Slow Clearance of Plasmodium falcip
- Page 147 and 148:
Gastroenteritis Caused by Norovirus
- Page 149 and 150:
Ebola Virus Stability on Surfaces a
- Page 151 and 152:
Ebola Virus Stability on Surfaces a
- Page 153 and 154:
Outbreak of Ciprofloxacin-Resistant
- Page 155 and 156:
Outbreak of S. sonnei, South KoreaT
- Page 157 and 158:
Rapidly Expanding Range of Highly P
- Page 159 and 160:
Cluster of Ebola Virus Disease, Bon
- Page 161 and 162:
Cluster of Ebola Virus Disease, Lib
- Page 163 and 164:
ANOTHER DIMENSIONThe Past Is Never
- Page 165 and 166:
Measles Epidemic, Boston, Massachus
- Page 167 and 168:
LETTERSInfluenza A(H5N6)Virus Reass
- Page 169 and 170:
LETTERSsystem (8 kb-span paired-end
- Page 171 and 172:
LETTERS3. Van Hong N, Amambua-Ngwa
- Page 173 and 174:
LETTERSTable. Prevalence of Bartone
- Page 175 and 176:
LETTERSavian influenza A(H5N1) viru
- Page 177 and 178:
LETTERSprovinces and a total of 200
- Page 179 and 180:
LETTERS7. Manian FA. Bloodstream in
- Page 181 and 182:
LETTERSforward projections. N Engl
- Page 183 and 184:
LETTERS3. Guindon S, Gascuel OA. Si
- Page 185 and 186:
BOOKS AND MEDIAin the port cities o
- Page 187 and 188:
ABOUT THE COVERNorth was not intere
- Page 189 and 190:
Earning CME CreditTo obtain credit,
- Page 191:
Emerging Infectious Diseases is a p