

9%20ECOGRAFIA%20ABDOMINAL%20COMO%20CUANDO%20DONDE

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
THE RENAL TRACT 177<br />
Xanthogranulomatous pyelonephritis (XGP)<br />
This condition (which gets its name from the yellow<br />
colour of the kidney) is the result of renal<br />
obstruction by calculi in the pelvicalyceal system.<br />
Frequently, a staghorn calculus is responsible.<br />
The kidney becomes chronically infected and<br />
the calyces enlarge and become filled with infected<br />
debris. The cortex may be eroded and thin (Fig.<br />
7.20).<br />
On ultrasound, these appearances are similar to<br />
TB or to a pyonephrosis. The latter is usually<br />
accompanied by a more severe, acute pain and<br />
fever whereas XGP or TB has a lower-grade,<br />
chronic pain.<br />
CT may differentiate TB from XGP and is also<br />
more sensitive to extrarenal spread of disease.<br />
Hydatid cysts<br />
The Echinococcus parasite spends part of its life<br />
cycle in dogs. The larvae may be transmitted to<br />
humans through contact with dog faeces, finding<br />
their way to the lungs, liver and, less frequently, the<br />
kidneys.<br />
The parasite forms a cyst which has a thickened<br />
wall, often with smaller, peripheral daughter cysts.<br />
Frequently the main cyst contains echoes.<br />
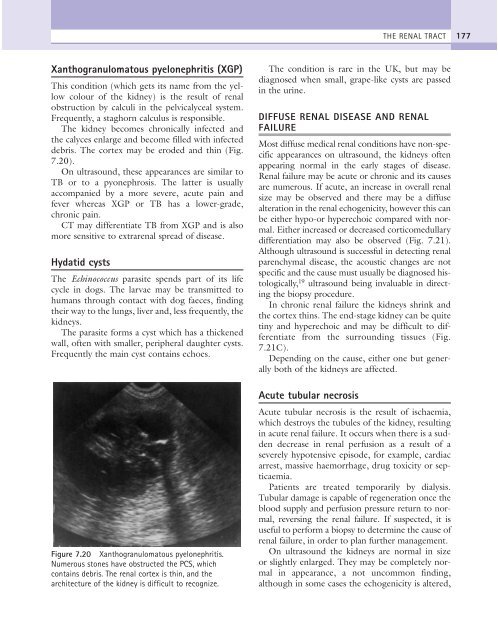
Figure 7.20 Xanthogranulomatous pyelonephritis.<br />
Numerous stones have obstructed the PCS, which<br />
contains debris. The renal cortex is thin, and the<br />
architecture of the kidney is difficult to recognize.<br />
The condition is rare in the UK, but may be<br />
diagnosed when small, grape-like cysts are passed<br />
in the urine.<br />
DIFFUSE RENAL DISEASE AND RENAL<br />
FAILURE<br />
Most diffuse medical renal conditions have non-specific<br />
appearances on ultrasound, the kidneys often<br />
appearing normal in the early stages of disease.<br />
Renal failure may be acute or chronic and its causes<br />
are numerous. If acute, an increase in overall renal<br />
size may be observed and there may be a diffuse<br />
alteration in the renal echogenicity, however this can<br />
be either hypo-or hyperechoic compared with normal.<br />
Either increased or decreased corticomedullary<br />
differentiation may also be observed (Fig. 7.21).<br />
Although ultrasound is successful in detecting renal<br />
parenchymal disease, the acoustic changes are not<br />
specific and the cause must usually be diagnosed histologically,<br />
19 ultrasound being invaluable in directing<br />
the biopsy procedure.<br />
In chronic renal failure the kidneys shrink and<br />
the cortex thins. The end-stage kidney can be quite<br />
tiny and hyperechoic and may be difficult to differentiate<br />
from the surrounding tissues (Fig.<br />
7.21C).<br />
Depending on the cause, either one but generally<br />
both of the kidneys are affected.<br />
Acute tubular necrosis<br />
Acute tubular necrosis is the result of ischaemia,<br />
which destroys the tubules of the kidney, resulting<br />
in acute renal failure. It occurs when there is a sudden<br />
decrease in renal perfusion as a result of a<br />
severely hypotensive episode, for example, cardiac<br />
arrest, massive haemorrhage, drug toxicity or septicaemia.<br />
Patients are treated temporarily by dialysis.<br />
Tubular damage is capable of regeneration once the<br />
blood supply and perfusion pressure return to normal,<br />
reversing the renal failure. If suspected, it is<br />
useful to perform a biopsy to determine the cause of<br />
renal failure, in order to plan further management.<br />
On ultrasound the kidneys are normal in size<br />
or slightly enlarged. They may be completely normal<br />
in appearance, a not uncommon finding,<br />
although in some cases the echogenicity is altered,