

9%20ECOGRAFIA%20ABDOMINAL%20COMO%20CUANDO%20DONDE

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
260<br />
ABDOMINAL ULTRASOUND<br />
R<br />
L<br />
R<br />
A<br />
B<br />
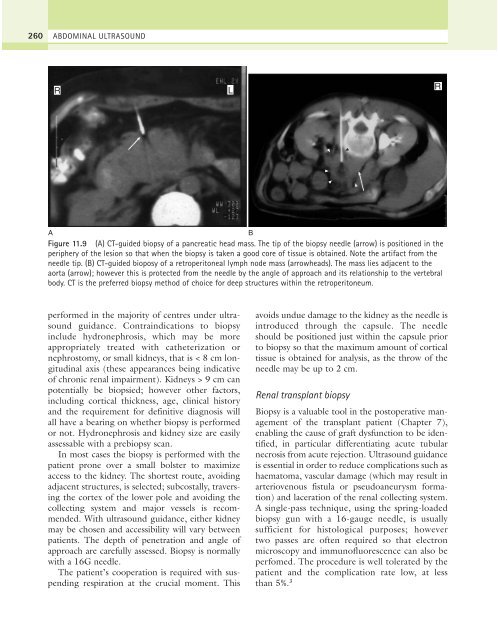
Figure 11.9 (A) CT-guided biopsy of a pancreatic head mass. The tip of the biopsy needle (arrow) is positioned in the<br />
periphery of the lesion so that when the biopsy is taken a good core of tissue is obtained. Note the artifact from the<br />
needle tip. (B) CT-guided bioposy of a retroperitoneal lymph node mass (arrowheads). The mass lies adjacent to the<br />
aorta (arrow); however this is protected from the needle by the angle of approach and its relationship to the vertebral<br />
body. CT is the preferred biopsy method of choice for deep structures within the retroperitoneum.<br />
performed in the majority of centres under ultrasound<br />
guidance. Contraindications to biopsy<br />
include hydronephrosis, which may be more<br />
appropriately treated with catheterization or<br />
nephrostomy, or small kidneys, that is < 8 cm longitudinal<br />
axis (these appearances being indicative<br />
of chronic renal impairment). Kidneys > 9 cm can<br />
potentially be biopsied; however other factors,<br />
including cortical thickness, age, clinical history<br />
and the requirement for definitive diagnosis will<br />
all have a bearing on whether biopsy is performed<br />
or not. Hydronephrosis and kidney size are easily<br />
assessable with a prebiopsy scan.<br />
In most cases the biopsy is performed with the<br />
patient prone over a small bolster to maximize<br />
access to the kidney. The shortest route, avoiding<br />
adjacent structures, is selected; subcostally, traversing<br />
the cortex of the lower pole and avoiding the<br />
collecting system and major vessels is recommended.<br />
With ultrasound guidance, either kidney<br />
may be chosen and accessibility will vary between<br />
patients. The depth of penetration and angle of<br />
approach are carefully assessed. Biopsy is normally<br />
with a 16G needle.<br />
The patient’s cooperation is required with suspending<br />
respiration at the crucial moment. This<br />
avoids undue damage to the kidney as the needle is<br />
introduced through the capsule. The needle<br />
should be positioned just within the capsule prior<br />
to biopsy so that the maximum amount of cortical<br />
tissue is obtained for analysis, as the throw of the<br />
needle may be up to 2 cm.<br />
Renal transplant biopsy<br />
Biopsy is a valuable tool in the postoperative management<br />
of the transplant patient (Chapter 7),<br />
enabling the cause of graft dysfunction to be identified,<br />
in particular differentiating acute tubular<br />
necrosis from acute rejection. Ultrasound guidance<br />
is essential in order to reduce complications such as<br />
haematoma, vascular damage (which may result in<br />
arteriovenous fistula or pseudoaneurysm formation)<br />
and laceration of the renal collecting system.<br />
A single-pass technique, using the spring-loaded<br />
biopsy gun with a 16-gauge needle, is usually<br />
sufficient for histological purposes; however<br />
two passes are often required so that electron<br />
microscopy and immunofluorescence can also be<br />
perfomed. The procedure is well tolerated by the<br />
patient and the complication rate low, at less<br />
than 5%. 3