

9%20ECOGRAFIA%20ABDOMINAL%20COMO%20CUANDO%20DONDE

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
THE PAEDIATRIC ABDOMEN 237<br />
mesenteric fixation of the small bowel to the<br />
posterior abdominal wall. This predisposes the small<br />
bowel to twisting (volving) around the mesenteric<br />
vascular axis, resulting in bowel obstruction and vascular<br />
compromise with a risk of infarction of most of<br />
the small bowel if the volvulus is not treated quickly.<br />
Following volvulus the child presents with acute<br />
pain and bile-stained vomiting. The bowel may<br />
intermittently twist and untwist, resulting in<br />
temporary alleviation of symptoms, which may<br />
make diagnosis more difficult.<br />
The definitive diagnosis is usually made fluoroscopically<br />
during an upper gastrointestinal contrast<br />
study. In malrotation the duodenal jejunal flexure is<br />
generally found to be lower and in a more medial<br />
position than is normal and if a volvulus has occurred<br />
a corkscrew appearance of the volved small bowel<br />
may be seen (Fig. 9.16). The proximal duodenum<br />
will be dilated secondary to the duodenal obstruction.<br />
Malrotation without volvulus may be suspected<br />
during a sonographic examination performed for<br />
intermittent abdominal pain due to the associated<br />
malposition of the mesenteric vessels and is best seen<br />
on colour Doppler sonography. The normal relationship<br />
of the superior mesenteric vein to the superior<br />
mesenteric artery is reversed, with the superior<br />
mesenteric vein lying anteriorly and/or to the left of<br />
the superior mesenteric artery. 33 However this finding<br />
is not always present and may occasionally be<br />
seen in normal individuals and therefore a contrast<br />
study is required for confirmation.<br />
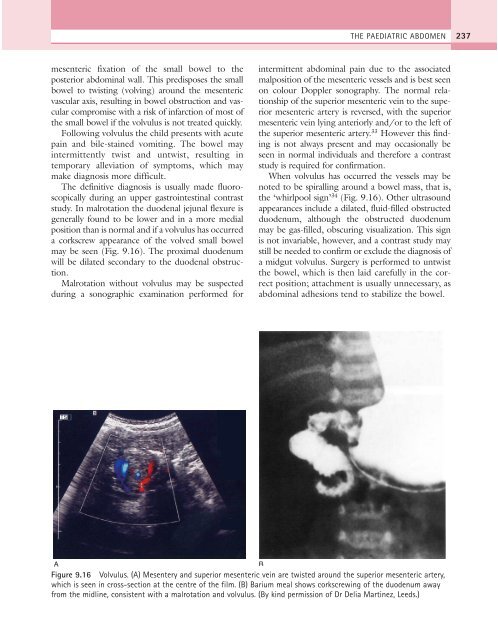
When volvulus has occurred the vessels may be<br />
noted to be spiralling around a bowel mass, that is,<br />
the ‘whirlpool sign’ 34 (Fig. 9.16). Other ultrasound<br />
appearances include a dilated, fluid-filled obstructed<br />
duodenum, although the obstructed duodenum<br />
may be gas-filled, obscuring visualization. This sign<br />
is not invariable, however, and a contrast study may<br />
still be needed to confirm or exclude the diagnosis of<br />
a midgut volvulus. Surgery is performed to untwist<br />
the bowel, which is then laid carefully in the correct<br />
position; attachment is usually unnecessary, as<br />
abdominal adhesions tend to stabilize the bowel.<br />
TS<br />
A<br />
B<br />
Figure 9.16 Volvulus. (A) Mesentery and superior mesenteric vein are twisted around the superior mesenteric artery,<br />
which is seen in cross-section at the centre of the film. (B) Barium meal shows corkscrewing of the duodenum away<br />
from the midline, consistent with a malrotation and volvulus. (By kind permission of Dr Delia Martinez, Leeds.)