éversibles. Malgré le faible nombre <strong>de</strong> cas rapportés,<strong>la</strong> neurapraxie médul<strong>la</strong>ire dorso-lombairesemble se distinguer <strong>de</strong> celle <strong>de</strong> siége cervical parl´absence <strong>de</strong> facteur favorisant, notamment d´uncanal médul<strong>la</strong>ire étroit constitutionnel ou d’uneinstabilité du canal vertébral, et par le dé<strong>la</strong>i <strong>de</strong>récupération plus long. D’autres étu<strong>de</strong>s à plus<strong>la</strong>rge échelle sont nécessaires afin d’éluci<strong>de</strong>r lesaspects pathomécaniques et physiopathologiques<strong>de</strong> cette entité encore peu connue.à propos d’une entite rare: <strong>la</strong> neurapraxie médul<strong>la</strong>ire dorso-lombaireTun Orthop 2008, Vol 1, N° 2V. réFérenCes1) Torg J.S, Pavlov H, Genuario S.E, Sennet B, Wisneski R.J,Robie B.H, and Jahre C. Neurapraxia of the cervical spinalcord with transient quadriplegia. J Bone and JointSurg 1986; 68A:1354-70.2) Scher AT. Spinal cord concussion in rugby p<strong>la</strong>yers. Am JSport Med 1991; 19:485-9.3) Andrews F.J. Transient cervical neurapraxia associatedwith cervical spine stenosis. Emerg Med J 2002; 19:172-3.4) Torg J.S, Naranja R.J, Pavlov H, Galinat B.J, Warren R,Stine R.A. The re<strong>la</strong>tionship of <strong>de</strong>velopmental narrowingof the cervical spinal canal to reversible and irreversibleinjury of the cervical spinal cord in football p<strong>la</strong>yers.An epi<strong>de</strong>miological study. J Bone Joint Surg 1996;78A:1308-14.5) Torg J.S, Thibault LE, Sennett B, et al. The pathomechanismsand pathophysiology of cervical spinal cord injury.Clin Orthop 1995; 321:259-69.6) Fehlings M.G, Farhadi H.F. Cervical stenosis, spinalcord neurapraxia, and the professional athlete. J NeurosurgSpine 2007; 6:354-5.7) Herzog RJ, Wiens JJ, Dillingham MF, et al. Normal cervicalspine morphometry and cervical spinal stenosis inasymptomatic professional football p<strong>la</strong>yers. Spine 1991;16:S178-89.209
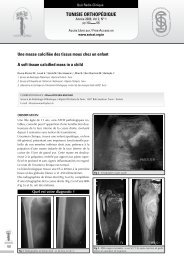
Quiz Radio-CliniqueTunisie OrThOpédiqueAnnée 2008, Vol 1, N° 2pp 210 212Accés Libre sur / Free Access onwww.<strong>sotcot</strong>.org.tnTorticolis chez un enfantTorticollis in childrenLouati H., 1 Douira W., 1 Sahli H., 1 Said W., 2 Ben Hassine L., 1 Smida M., 2 Ben Ghachem M., 2 Bel<strong>la</strong>gha I. 11 Service <strong>de</strong> Radiopédiatrie. Hôpital d’Enfants <strong>de</strong> Tunis. Bab Saadoun 1007 - Tunis2 Service d’Orthopédie <strong>de</strong> l’enfant et l’Adolescent. Hôpital d’Enfants <strong>de</strong> Tunis. Bab Saadoun 1007 - TunisCORRESPONDANCE : hé<strong>la</strong> louatiService <strong>de</strong> Radiopédiatrie. Hôpital d’Enfants <strong>de</strong> Tunis. P<strong>la</strong>ce Bab Saadoun 1007 Jabbari TunisE-mail : hallou<strong>la</strong>_louati@yahoo.fri. oBserVationIl s’agit d’un enfant âgé <strong>de</strong> 12 ans sans antécé<strong>de</strong>ntspathologiques connus, hospitalisé <strong>pour</strong>prise en charge d’un torticolis droit atraumatique(Fig 1).Figure 2a : Radiographie du rachis cervical <strong>de</strong> face Chevauchementavec aspect caché <strong>de</strong> <strong>la</strong> facette articu<strong>la</strong>ire droite.Figure 1: Torticolis droit chez un enfant <strong>de</strong> 12 ans210La symptomatologie remonte à quatre jours avantson hospitalisation, marquée par l’apparition brutaled’un torticolis sans notion <strong>de</strong> traumatisme ni<strong>de</strong> fièvre.A l’examen, il y avait une contracture <strong>de</strong>s musclesspinaux et du muscle sterno-cleido-mastoidiengauche avec une légère sensibilité à <strong>la</strong> palpation<strong>de</strong>s épineuses <strong>de</strong> C2 et C3.Des radiographies du rachis cervical <strong>de</strong> face (Fig2a) et bouche ouverte (Fig 2b) ont été réaliséessuivies d’une tomo<strong>de</strong>nsitométrie du rachis cervical(Fig 3a-d).Figure 2b : Radiographie du rachis cervical <strong>de</strong> face bouche ouverte.Désaxation et excentration <strong>de</strong> l’odontoi<strong>de</strong> par rapport aux masses <strong>la</strong>térales.La masse <strong>la</strong>térale droite <strong>de</strong> C1 paraît plus <strong>la</strong>rge et plus proche <strong>de</strong><strong>la</strong> ligne médiane que son homologue contro<strong>la</strong>téral
- Page 2 and 3:
Tunisie OrThOpédiqueOrgane Offi ci
- Page 4 and 5:
SommaireTunisie OrThOpédiqueAnnée
- Page 6 and 7:
ÉditorialTunisie OrThOpédiqueAnn
- Page 8 and 9:
Orthopédie signifie, d’après le
- Page 10:
Conférence d’ActualitéTunisie O
- Page 14:
les chances de mise en évidence de
- Page 19:
Tun Orthop 2008, Vol 1, N° 2124Ben
- Page 22 and 23:
• Douleurs articulaires exacerbé
- Page 24 and 25:
d’une antibiothérapie par voie o
- Page 28 and 29:
57) Yagupsky P, Press J. Use of the
- Page 30 and 31:
i. teChnique ChirurGiCaleL’interv
- Page 32:
Article OriginalTunisie OrThOpédiq
- Page 35:
Tun Orthop 2008, Vol 1, N° 2140Zar
- Page 38 and 39:
Article OriginalTunisie OrThOpédiq
- Page 40 and 41:
Résultats de l’ostéotomie tibia
- Page 42 and 43:
Résultats de l’ostéotomie tibia
- Page 44 and 45:
Résultats de l’ostéotomie tibia
- Page 46 and 47:
i. introduCtionLe traitement de l
- Page 48 and 49:
C- Résultats cliniquesAu dernier r
- Page 50 and 51:
elation entre la position de la but
- Page 52 and 53:
i. introduCtionLa dysplasie cotylo
- Page 54 and 55: Résultats du traitement de la dysp
- Page 56 and 57: maintiendra tout au long de la croi
- Page 59 and 60: écrire ou périrécrire pour s’
- Page 61 and 62: Tun Orthop 2008, Vol 1, N° 2Zrig M
- Page 65 and 66: Tun Orthop 2008, Vol 1, N° 2170Zri
- Page 67 and 68: Tun Orthop 2008, Vol 1, N° 2172Bou
- Page 69 and 70: Tun Orthop 2008, Vol 1, N° 2Bouatt
- Page 72 and 73: Hardouin P, Jeanfils J et al. : Gen
- Page 74 and 75: i. introduCtionii. matériel et mé
- Page 76 and 77: partiellement ou, dans de rare cas,
- Page 78 and 79: Note TechniqueTunisie OrThOpédique
- Page 80 and 81: obtenue à un mois post-opératoire
- Page 82 and 83: Cas CliniqueTunisie OrThOpédiqueAn
- Page 84 and 85: L’ostéosarcome intra-médullaire
- Page 87 and 88: Tun Orthop 2008, Vol 1, N° 2Ayadi
- Page 89 and 90: Tun Orthop 2008, Vol 1, N° 2Ayadi
- Page 91 and 92: Tun Orthop 2008, Vol 1, N° 2Mnif H
- Page 93 and 94: Tun Orthop 2008, Vol 1, N° 2Mnif H
- Page 95 and 96: Tun Orthop 2008, Vol 1, N° 2Kandar
- Page 97 and 98: Cas CliniqueTunisie OrThOpédiqueAn
- Page 99 and 100: Tun Orthop 2008, Vol 1, N° 2204Gua
- Page 101 and 102: Cas CliniqueTunisie OrThOpédiqueAn
- Page 103: Tun Orthop 2008, Vol 1, N° 2208Say
- Page 107 and 108: Tun Orthop 2008, Vol 1, N° 2Louati
- Page 109 and 110: Articles ImmigrésTunisie OrThOpéd
- Page 111 and 112: Tun Orthop 2008, Vol 1, N° 2Articl
- Page 113 and 114: Tun Orthop 2008, Vol 1, N° 2Articl
- Page 115 and 116: Articles sous MicroscopeTunisie OrT
- Page 117 and 118: Tun Orthop 2008, Vol 1, N° 2222Art
- Page 119 and 120: Tun Orthop 2008, Vol 1, N° 2Articl
- Page 121 and 122: Tun Orthop 2008, Vol 1, N° 2226Art
- Page 123 and 124: Tun Orthop 2008, Vol 1, N° 2Articl
- Page 125: Recommandations aux AuteursTunisie