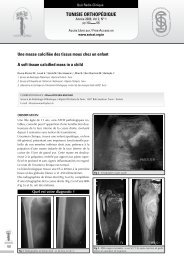
Article OriginalTunisie OrThOpédiqueAnnée 2008, Vol 1, N° 2pp 171 177Accés Libre sur / Free Access onwww.<strong>sotcot</strong>.org.tnrésultats du traitement chirurgical <strong>de</strong>s ostéomes neurogènes <strong>de</strong> <strong>la</strong> hanche.à propos <strong>de</strong> 30 casheterotopic ossification of the hip. results of surgery about 30 casesBouattour K., Boughamoura H., Mseddi M., Naija W., Sia<strong>la</strong> A., Dahmene J., Ben Ayeche M.L.Service d’orthopédie, hôpital Sahloul, Sousse, TunisieCORRESPONDANCE : hatem BouGhamouraService d’Orthopédie et Traumatologie. CHU Sahloul Sousse. Route Ceinture Sahloul 4054 SOUSSE.E-mail : Hatem.boughammoura@rns.tnrésuméIntroductionNous rapportons dans ce travail rétrospectif les résultats anatomiques etfonctionnels <strong>de</strong> 30 cas d’ostéomes neurogènes <strong>de</strong> <strong>la</strong> hanche chez 21 patients,traités par résection arthrolyse suivie <strong>de</strong> rééducation.Matériel et métho<strong>de</strong>sIl s’agissait <strong>de</strong> patients jeunes (33 ans en moyenne) avec une hanche ankyloséedans 80% <strong>de</strong>s cas. L’ostéome faisait suite à un coma prolongé <strong>pour</strong> 18patients et à une atteinte médul<strong>la</strong>ire <strong>pour</strong> les 3 autres. L’atteinte <strong>de</strong> <strong>la</strong> hancheétait bi<strong>la</strong>térale dans 11 cas (dont 9 ont été opérés <strong>de</strong>s <strong>de</strong>ux cotés), associéeà une atteinte du genou (31,5%), ou du cou<strong>de</strong> (25,8%) <strong>pour</strong> un nombre totald’ostéomes <strong>de</strong> 89. Le siège <strong>de</strong> l’ostéome était circonférentiel dans 8 cas. Onzepatients (61%) étaient c<strong>la</strong>ssés sta<strong>de</strong> III <strong>de</strong> Gar<strong>la</strong>nd. Les patients ont été opérésaprès un dé<strong>la</strong>i moyen <strong>de</strong> 36 mois, après maturation <strong>de</strong> l’ostéome jugée à <strong>la</strong>scintigraphie. L’intervention a consisté en une résection arthrolyse, associéedans 6 cas à une arthrop<strong>la</strong>stie totale.RésultatsLes résultats ont été analysés à 34 mois <strong>de</strong> recul moyen. Les complicationscomportaient 4 fractures proximales du fémur, 2 infections et 4 instabilités dontl’évolution a été favorable. Cependant, un patient est décédé <strong>de</strong>s suites d’unelésion vascu<strong>la</strong>ire. L’ostéome a récidivé chez 3 patients (5 hanches), toujoursprécocement. Ces 3 patients gardaient <strong>de</strong>s séquelles neurologiques.Le résultat fonctionnel montre un gain absolu moyen en flexion <strong>de</strong> 60,5°. Sept<strong>de</strong>s 9 patients grabataires et les 6 patients confinés à <strong>la</strong> chaise rou<strong>la</strong>nte ontpu remarcher.ConclusionLa prise en charge <strong>de</strong>s ostéomes <strong>de</strong> hanche reste difficile, en particulier lesostéomes circonférentiels. La chirurgie ne doit pas nécessairement attendre<strong>la</strong> maturation <strong>de</strong> l’ostéome mais plutôt <strong>la</strong> stabilisation neurologique.ABsTrAcTIntroductionIn this retrospective study, we report the anatomic and functional results of 30cases of hip heterotopic ossification of 21 patients treated by resection arthrolysisfollowed by rehabilitation.Material and MethodsWe report cases of young patients (33 years in average) with non functionalhip in 80% of the cases. The heterotopic ossification was discovered after aprolonged coma for 18 patients and a spinal injury for the 3 others.Hips localisation of the heterotopic ossification was bi<strong>la</strong>teral in 11 cases (9was operated on the two sites), and was associated with knee localisation(31.5%), or elbow localisation (21.8%) for a complete number of 89. The localisationof the heterotopic ossification was circumferential in 8 cases. Elevenpatients (61%) were c<strong>la</strong>ssified gra<strong>de</strong> III of Gar<strong>la</strong>nd. The surgery was performedafter heterotopic ossification maturation proved by scintigraphy (after 36months in average).The surgery was an arthrolysis resection, associated witha total arthrop<strong>la</strong>sty in 6 cases.ResultsThe results was analysed after 34 months in average. The complications were: 4proximal fractures of the femur, 2 <strong>de</strong>ep infections and 4 instabilities which evolutionwas favourable. One patient died by a vascu<strong>la</strong>r injury. The heterotopic ossificationwas reccured in 3 patients (in 5 hips), and it was always few time aftersurgery. These 3 patients have <strong>de</strong>veloped neurological complication.The functional result showed an improvement in flexion of 60.5° in average.Seven of the 9 bedrid<strong>de</strong>n invalid’s patients and the 6 confined to the wheelchairwere able to walk again.ConclusionThe coverage of the heterotopic ossification remain difficult, particu<strong>la</strong>rly thosewho are circumferential. We should not necessarily wait for the ossification maturationto perform surgery, but it’s important to wait for the neurological stabilisation.mots clés : hanche, ostéome neurogène, résection -arthrolyse, résultat fonctionnel,traumatisme crânienKey words : hip, heterotopic ossification, resection-arthrolysis, functional result,head injury171
Tun Orthop 2008, Vol 1, N° 2172Bouattour K et al.i. introduCtionLes para-ostéo-arthropathies neurogènes ou ostéomesneurogènes, sont <strong>de</strong>s ossifications ectopiques,juxta articu<strong>la</strong>ires, apparaissant essentiellementchez <strong>de</strong>s patients paraplégiques outraumatisés crânien graves, mais aussi au coursd’affection neurologiques très diverses [12, 13].Les ostéomes surviennent uniquement dans lesterritoires atteints neurologiquement et se localisentquasi exclusivement autour <strong>de</strong>s grosses articu<strong>la</strong>tionsproximales <strong>de</strong>s membres : hanches,cou<strong>de</strong>s, genoux, épaules. Leur retentissementfonctionnel est considérable.La résection chirurgicale <strong>de</strong> l’ostéome représenteactuellement <strong>la</strong> seule alternative. Mais il s’agitd’une chirurgie difficile réalisée sur un terrainparticulier (séquelles neurologiques, nombre importantd’ostéomes). Elle doit être entourée d’unerééducation appropriée.Peu d’étu<strong>de</strong>s ont été consacrées aux résultats <strong>de</strong><strong>la</strong> chirurgie <strong>de</strong>s ostéomes <strong>de</strong> <strong>la</strong> hanche. La situationprofon<strong>de</strong> <strong>de</strong> l’articu<strong>la</strong>tion, <strong>la</strong> présence d’attitu<strong>de</strong>svicieuses et d’ostéomes circonférentielsexpliquent aussi les difficultés <strong>de</strong> prise en charge.Par ailleurs, le risque <strong>de</strong> récidive <strong>de</strong> l’ostéomeaprès traitement chirurgical ainsi que le risqued’instabilité <strong>de</strong> <strong>la</strong> hanche, amènent à envisagerune stratégie thérapeutique bien codifiée.Nous avons revu 30 cas d’ostéomes <strong>de</strong> <strong>la</strong> hanche,opérés puis suivis en rééducation fonctionnelle,dans le but d’évaluer les résultats anatomiqueset fonctionnels et <strong>de</strong> préciser les facteurs <strong>de</strong> récidive.ii. patients et métho<strong>de</strong>sA- PatientsEntre 1992 et 2004, 21 patients ont été opérés<strong>pour</strong> un ostéome <strong>de</strong> hanche dont 9 <strong>de</strong>s <strong>de</strong>ux cotés.Il s’agissait <strong>de</strong> 18 hommes et 3 femmes dontl’age moyen au moment <strong>de</strong> l’intervention était<strong>de</strong> 33 ans (20-50ans).L’ostéome faisait suite à une atteinte médul<strong>la</strong>irechez 3 patients (5 hanches) et à un coma prolongéchez 18 patients (25 hanches) : un traumatismecrânien grave dans 14 cas, une thrombophlébitecérébrale dans un cas, un choc septiquedans un cas, une méningite tuberculeuse dansun cas et une détresse respiratoire compliquantune myasthénie dans un cas. La durée moyennedu coma était <strong>de</strong> 35 jours (25-90 jours).Onze patients avaient une localisation bi<strong>la</strong>térale(dont 9 ont été opérés, successivement, sur les<strong>de</strong>ux cotés). Les autres articu<strong>la</strong>tions étaient aussiconcernées par les ostéomes : Le genou (31,5%<strong>de</strong>s patients), le cou<strong>de</strong> (25,8%) et l’épaule(4,5%). Le nombre total d’ostéomes <strong>pour</strong> les 21patients était <strong>de</strong> 89 avec <strong>de</strong>s extrêmes <strong>de</strong> 1 à 8par patient.Les circonstances <strong>de</strong> découverte <strong>de</strong> l’ostéomeétaient une rai<strong>de</strong>ur articu<strong>la</strong>ire ou une ankylose.La mobilité <strong>de</strong> <strong>la</strong> hanche était très limitée dans6 cas (dont 3 dans un secteur non fonctionnel)et nulle (hanche ankylosée) dans 24 cas (80%).L’évaluation fonctionnelle <strong>de</strong>s blessés médul<strong>la</strong>iresmontrait <strong>de</strong>ux patients cotés ASIA «A» etun patient coté ASIA «D».L’évaluation <strong>de</strong>s patients après coma s’est baséesur le G<strong>la</strong>sgow coma scale (Tableau 1) et sur <strong>la</strong>c<strong>la</strong>ssification <strong>de</strong> Gar<strong>la</strong>nd (Tableau 2).tableau 1 : Échelle <strong>de</strong> G<strong>la</strong>sgow (Traumatisés crâniens)Gra<strong>de</strong> handicapBonne récupération : retour à <strong>la</strong> vie normale +/- légère déficience1motrice ou mentaleHandicap modéré (autorisant une indépendance dans <strong>la</strong> vie quotidienne)23 Handicap sévère nécessitant l’assistance d’une tierce personne4 État végétatif5 Décèstableau 2 : C<strong>la</strong>ssification <strong>de</strong> Gar<strong>la</strong>nd (Traumatisés crâniens)sta<strong>de</strong> déficitI Déficit fonctionnel et cognitif minimeII Déficit fonctionnel modéré. Déficit cognitif minimeIII Déficit fonctionnel sévère. Déficit cognitif minimeDéficit fonctionnel minime ou modéréIVDéficit cognitif modéré ou sévèreDéficit fonctionnel sévèreVDéficit cognitif modéré ou sévèreEn se basant sur le G<strong>la</strong>sgow coma scale, 10 patients (55%)étaient c<strong>la</strong>ssés gra<strong>de</strong> 3 soit un handicap sévère avec tiercepersonne nécessaire <strong>pour</strong> les gestes <strong>de</strong> <strong>la</strong> vie quotidienne et8 patients (38%) avaient un handicap gra<strong>de</strong> 2 ou modéré.L’évaluation selon <strong>la</strong> c<strong>la</strong>ssification <strong>de</strong> Gar<strong>la</strong>nd montrait que7 patients (39%) étaient c<strong>la</strong>ssés sta<strong>de</strong> II et 11 patients (61%)étaient c<strong>la</strong>ssés sta<strong>de</strong> III (déficit fonctionnel sévère et déficitcognitif minime).Au total, six patients gardaient un déficit moteur: paraplégie complète (1 cas), tétra-parésie (1cas), para-parésie (1 cas) et hémi-parésie (3 cas).Il n’ y avait aucune localisation contro<strong>la</strong>térale audéficit neurologique.Ainsi, sur le p<strong>la</strong>n fonctionnel, 9 patients étaientgrabataires et totalement dépendants d’unetierce personne, 6 patients étaient confinés à <strong>la</strong>chaise rou<strong>la</strong>nte, 5 patients marchaient à l’ai<strong>de</strong><strong>de</strong> <strong>de</strong>ux cannes bé<strong>qui</strong>lles et 1 patient marchaitsans canne mais avec boiterie.Le siège <strong>de</strong> l’ostéome a été analysé sur les radiographiesstandard et sur l’examen tomo<strong>de</strong>nsitométrique,réalisés dans tous les cas. L’ostéomeétait antérieur dans 17 cas (57%), postérieur dans5 cas (17%) et circonférentiel dans 8 cas (26%).L’interligne articu<strong>la</strong>ire était aminci dans 8 cas.
- Page 2 and 3:
Tunisie OrThOpédiqueOrgane Offi ci
- Page 4 and 5:
SommaireTunisie OrThOpédiqueAnnée
- Page 6 and 7:
ÉditorialTunisie OrThOpédiqueAnn
- Page 8 and 9:
Orthopédie signifie, d’après le
- Page 10:
Conférence d’ActualitéTunisie O
- Page 14:
les chances de mise en évidence de
- Page 19: Tun Orthop 2008, Vol 1, N° 2124Ben
- Page 22 and 23: • Douleurs articulaires exacerbé
- Page 24 and 25: d’une antibiothérapie par voie o
- Page 28 and 29: 57) Yagupsky P, Press J. Use of the
- Page 30 and 31: i. teChnique ChirurGiCaleL’interv
- Page 32: Article OriginalTunisie OrThOpédiq
- Page 35: Tun Orthop 2008, Vol 1, N° 2140Zar
- Page 38 and 39: Article OriginalTunisie OrThOpédiq
- Page 40 and 41: Résultats de l’ostéotomie tibia
- Page 42 and 43: Résultats de l’ostéotomie tibia
- Page 44 and 45: Résultats de l’ostéotomie tibia
- Page 46 and 47: i. introduCtionLe traitement de l
- Page 48 and 49: C- Résultats cliniquesAu dernier r
- Page 50 and 51: elation entre la position de la but
- Page 52 and 53: i. introduCtionLa dysplasie cotylo
- Page 54 and 55: Résultats du traitement de la dysp
- Page 56 and 57: maintiendra tout au long de la croi
- Page 59 and 60: écrire ou périrécrire pour s’
- Page 61 and 62: Tun Orthop 2008, Vol 1, N° 2Zrig M
- Page 65: Tun Orthop 2008, Vol 1, N° 2170Zri
- Page 69 and 70: Tun Orthop 2008, Vol 1, N° 2Bouatt
- Page 72 and 73: Hardouin P, Jeanfils J et al. : Gen
- Page 74 and 75: i. introduCtionii. matériel et mé
- Page 76 and 77: partiellement ou, dans de rare cas,
- Page 78 and 79: Note TechniqueTunisie OrThOpédique
- Page 80 and 81: obtenue à un mois post-opératoire
- Page 82 and 83: Cas CliniqueTunisie OrThOpédiqueAn
- Page 84 and 85: L’ostéosarcome intra-médullaire
- Page 87 and 88: Tun Orthop 2008, Vol 1, N° 2Ayadi
- Page 89 and 90: Tun Orthop 2008, Vol 1, N° 2Ayadi
- Page 91 and 92: Tun Orthop 2008, Vol 1, N° 2Mnif H
- Page 93 and 94: Tun Orthop 2008, Vol 1, N° 2Mnif H
- Page 95 and 96: Tun Orthop 2008, Vol 1, N° 2Kandar
- Page 97 and 98: Cas CliniqueTunisie OrThOpédiqueAn
- Page 99 and 100: Tun Orthop 2008, Vol 1, N° 2204Gua
- Page 101 and 102: Cas CliniqueTunisie OrThOpédiqueAn
- Page 103 and 104: Tun Orthop 2008, Vol 1, N° 2208Say
- Page 105 and 106: Quiz Radio-CliniqueTunisie OrThOpé
- Page 107 and 108: Tun Orthop 2008, Vol 1, N° 2Louati
- Page 109 and 110: Articles ImmigrésTunisie OrThOpéd
- Page 111 and 112: Tun Orthop 2008, Vol 1, N° 2Articl
- Page 113 and 114: Tun Orthop 2008, Vol 1, N° 2Articl
- Page 115 and 116: Articles sous MicroscopeTunisie OrT
- Page 117 and 118:
Tun Orthop 2008, Vol 1, N° 2222Art
- Page 119 and 120:
Tun Orthop 2008, Vol 1, N° 2Articl
- Page 121 and 122:
Tun Orthop 2008, Vol 1, N° 2226Art
- Page 123 and 124:
Tun Orthop 2008, Vol 1, N° 2Articl
- Page 125:
Recommandations aux AuteursTunisie