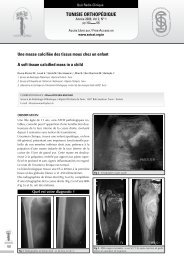
Cas CliniqueTunisie OrThOpédiqueAnnée 2008, Vol 1, N° 2pp 187 190Accés Libre sur / Free Access onwww.<strong>sotcot</strong>.org.tnL’ostéosarcome intra-médul<strong>la</strong>ire <strong>de</strong> bas gra<strong>de</strong>.une entité rare et déroutanteLow gra<strong>de</strong> intra-osseous osteosarcoma.A rare and misleading entityHannachi Sassi S., 1 Doghri R., 1 Abbes I., 1 Mrad K., 1 Ben S<strong>la</strong>ma S., 1 Dhouib R., 1 Driss M., 1 Azaeiz H., 1 Cherif M.R., 2 M’barek M., 2 Ben Romdhnae K. 11. Laboratoire d’Anatomie et <strong>de</strong> Cytologie Pathologiques. Institut Sa<strong>la</strong>h Azaiez, Bab Saadoun, 1006 Tunis, Tunisie2. Service <strong>de</strong> Chirurgie Orthopédique et Traumatologique. Hôpital Aziza Othmana. P<strong>la</strong>ce du Gouvernement Tunis. TunisieCORRESPONDANCE : samia hannaChi sassiVil<strong>la</strong> 7 Impasse 3 Rue <strong>de</strong>s Mères <strong>de</strong> Tunisie. Les jardins d’El Menzah El Manar I, 2092 Tunis - Tunisie.E-mail : samia.hannachi@rns.tnrésuméL’ostéosarcome intra-médul<strong>la</strong>ire <strong>de</strong> bas gra<strong>de</strong> (OIBD) est une variante rare d’ostéosarcome(1 à 2% <strong>de</strong>s ostéosarcomes) d’évolution indolente par rapport à l’ostéosarcomeconventionnel. Son diagnostic histologique est parfois difficile car ilpeut ressembler à un ostéosarcome juxta-cortical, une dysp<strong>la</strong>sie fibreuse ou à unfibrome <strong>de</strong>smop<strong>la</strong>stique. Mais, <strong>la</strong> confrontation radiologique et histologique est indispensableet permet souvent <strong>de</strong> redresser le diagnostic.Nous rapportons un cas et étudions les aspects anatomo-cliniques <strong>de</strong> cette entitérare en insistant sur les problèmes <strong>de</strong> diagnostic différentiel.ABsTrAcTLow gra<strong>de</strong> intra-osseous osteosarcoma (LGIO) is a very rare and painlessform of osteosarcoma (1 to 2% of osteosarcomas). The histological diagnosisis sometimes difficult because of its simi<strong>la</strong>rities to juxtacortical osteosarcoma,fibrous dysp<strong>la</strong>sia or <strong>de</strong>smop<strong>la</strong>stic fibroma. The confrontation between imagingand histopathology is helpful to the exact diagnosis.We report here a case of LGIO osteosarcoma and we will <strong>de</strong>scribe the anatomo-clinica<strong>la</strong>spects of this entity and stress on diagnosis problems.mots-clés: ostéosarcome intra-médul<strong>la</strong>ire, bas gra<strong>de</strong>, diagnostic différentielKeywords: osteosarcoma, low gra<strong>de</strong>, intra-osseous187
Tun Orthop 2008, Vol 1, N° 2Hannachi Sassi S et al.i. introduCtionL’ostéosarcome est actuellement divisé en plusieursvariétés différentes selon les données cliniques,radiologiques et histologiques. Même si <strong>la</strong>plupart <strong>de</strong>s ostéosarcomes sont <strong>de</strong> haut gra<strong>de</strong> <strong>de</strong>malignité, il est important <strong>de</strong> reconnaître l’ostéosarcome<strong>de</strong> bas gra<strong>de</strong> intra-osseux et <strong>de</strong> surface.L’ostéosarcome <strong>de</strong> bas gra<strong>de</strong> <strong>de</strong> surface, encoreappelé ostéosarcome parostéal (ou juxta-cortical),est <strong>de</strong> bon pronostic et diffère cliniquementet histologiquement <strong>de</strong> l’ostéosarcome conventionnel.Cependant, l’ostéosarcome intra-osseux<strong>de</strong> bas gra<strong>de</strong> (OIBD) est une variante rare d’ostéosarcomed’évolution indolente dont le diagnosticest souvent difficile [1].du grand trochanter. En bas, <strong>la</strong> tumeur arrivait auniveau <strong>de</strong> <strong>la</strong> p<strong>la</strong>que osseuse sous-chondrale auniveau du condyle externe, alors qu’elle respectait<strong>la</strong> <strong>partie</strong> inférieure et postérieure du condyleinterne. Il existait une extension tumorale dans les<strong>partie</strong>s molles prédominant en arrière et en externemais également présente en avant où ellerestait à distance du tendon quadricipital. L’articu<strong>la</strong>tiondu genou, les axes vascu<strong>la</strong>ires et nerveuxn’étaient pas envahis (Fig 2).188ii. oBserVationIl s’agit d’une femme âgée <strong>de</strong> 28 ans, sans antécé<strong>de</strong>ntspathologiques notables, <strong>qui</strong> était hospitalisée<strong>pour</strong> <strong>de</strong>s douleurs persistantes <strong>de</strong> l’extrémitéinférieure du genou droit évoluant <strong>de</strong>puisun an, en <strong>de</strong>hors <strong>de</strong> tout contexte inf<strong>la</strong>mmatoireet traumatique. L’examen clinique révé<strong>la</strong>it unedouleur à <strong>la</strong> palpation sans tuméfaction associée,localisée au niveau <strong>de</strong> l’extrémité inférieure dufémur droit. La mobilité du genou et <strong>de</strong> <strong>la</strong> hancheétait normale. Il n’y avait pas <strong>de</strong> signes inf<strong>la</strong>mmatoires,ni d’adénopathies loco-régionales. Le reste<strong>de</strong> l’examen orthopédique et le bi<strong>la</strong>n biologiqueétaient normaux.Les radiographies standards mettaient en évi<strong>de</strong>nceune tumeur con<strong>de</strong>nsante <strong>de</strong> l’extrémitéinférieure du fémur droit, comb<strong>la</strong>nt <strong>la</strong> cavité médul<strong>la</strong>ireavec un envahissement <strong>de</strong>s <strong>partie</strong>s molles(Fig 1).Figure 1 : Radiographie standard: tumeur con<strong>de</strong>nsante <strong>de</strong> l’extrémitéinférieure du fémur droit, comb<strong>la</strong>nt <strong>la</strong> cavité médul<strong>la</strong>ire avec un envahissement<strong>de</strong>s <strong>partie</strong>s mollesL’IRM du fémur droit objectivait une lésion centroosseuseépiphyso-métaphyso-diaphysaire étenduesur 11 cm faite d’os compacte en hyposignal T1et T2 (témoignant <strong>de</strong> son caractère con<strong>de</strong>nsant) etcontenant par endroits <strong>de</strong>s zones hémorragiquesen hyposignal T1 et T2. La limite supérieure <strong>de</strong><strong>la</strong> tumeur se situait à 32,5 cm du bord supérieurFigure 2 : IRM du fémur droit: lésion centro-osseuse épiphyso-métaphyso-diaphysaireétendue faite d’os compacte en hyposignal T1 et T2(témoignant <strong>de</strong> son caractère con<strong>de</strong>nsant)Le bi<strong>la</strong>n d’extension générale (TDM thoraco-abdominaleet scintigraphy osseuse) ne montrait pas<strong>de</strong> localisations secondaires.Une biopsie chirurgicale, réalisait à <strong>de</strong>ux reprises,avait conclu à un ostéosarcome juxta-cortica<strong>la</strong>vec envahissement secondaire <strong>de</strong> <strong>la</strong> médul<strong>la</strong>ire.Une résection en bloc <strong>de</strong> <strong>la</strong> tumeur, sans chimiothérapiepré-opératoire, suivie d’une prothèsemassive ont été réalisées. La pièce opératoiremesurait 17/10/7 cm et comportait une sectionchirurgicale passant par <strong>la</strong> région diaphysaire.Elle était recouverte <strong>de</strong> tissu mou du coté internesur 15/6 cm comportant en surface un <strong>la</strong>mbeaucutané <strong>de</strong> 9/1,5 cm. Une section selon p<strong>la</strong>n frontalet médian a été réalisée montrant que <strong>la</strong> quasi-totalité<strong>de</strong> <strong>la</strong> cavité médul<strong>la</strong>ire était occupéepar une tumeur d’aspect b<strong>la</strong>nchâtre ossifiée, <strong>de</strong>contours irréguliers et s’étendant sur une hauteur<strong>de</strong> 12, 5 cm. Elle était distante <strong>de</strong> 3,5 cm <strong>de</strong> <strong>la</strong>limite <strong>de</strong> résection chirurgicale et <strong>de</strong> 0,7 cm ducarti<strong>la</strong>ge <strong>de</strong>s condyles fémoraux. La tumeur rompaitfocalement <strong>la</strong> corticale avec présence <strong>de</strong> 3nodules tumoraux sous-périostés dont 2 médioexternes<strong>de</strong> 0,5 et 1,5 cm <strong>de</strong> grand axe et 1 médio-interne<strong>de</strong> 1,5 cm <strong>de</strong> grand axe. Il existait unnodule tumoral dans les <strong>partie</strong>s molles postérointernesmesurant 4 cm <strong>de</strong> grand axe (Fig 3).
- Page 2 and 3:
Tunisie OrThOpédiqueOrgane Offi ci
- Page 4 and 5:
SommaireTunisie OrThOpédiqueAnnée
- Page 6 and 7:
ÉditorialTunisie OrThOpédiqueAnn
- Page 8 and 9:
Orthopédie signifie, d’après le
- Page 10:
Conférence d’ActualitéTunisie O
- Page 14:
les chances de mise en évidence de
- Page 19:
Tun Orthop 2008, Vol 1, N° 2124Ben
- Page 22 and 23:
• Douleurs articulaires exacerbé
- Page 24 and 25:
d’une antibiothérapie par voie o
- Page 28 and 29:
57) Yagupsky P, Press J. Use of the
- Page 30 and 31:
i. teChnique ChirurGiCaleL’interv
- Page 32: Article OriginalTunisie OrThOpédiq
- Page 35: Tun Orthop 2008, Vol 1, N° 2140Zar
- Page 38 and 39: Article OriginalTunisie OrThOpédiq
- Page 40 and 41: Résultats de l’ostéotomie tibia
- Page 42 and 43: Résultats de l’ostéotomie tibia
- Page 44 and 45: Résultats de l’ostéotomie tibia
- Page 46 and 47: i. introduCtionLe traitement de l
- Page 48 and 49: C- Résultats cliniquesAu dernier r
- Page 50 and 51: elation entre la position de la but
- Page 52 and 53: i. introduCtionLa dysplasie cotylo
- Page 54 and 55: Résultats du traitement de la dysp
- Page 56 and 57: maintiendra tout au long de la croi
- Page 59 and 60: écrire ou périrécrire pour s’
- Page 61 and 62: Tun Orthop 2008, Vol 1, N° 2Zrig M
- Page 65 and 66: Tun Orthop 2008, Vol 1, N° 2170Zri
- Page 67 and 68: Tun Orthop 2008, Vol 1, N° 2172Bou
- Page 69 and 70: Tun Orthop 2008, Vol 1, N° 2Bouatt
- Page 72 and 73: Hardouin P, Jeanfils J et al. : Gen
- Page 74 and 75: i. introduCtionii. matériel et mé
- Page 76 and 77: partiellement ou, dans de rare cas,
- Page 78 and 79: Note TechniqueTunisie OrThOpédique
- Page 80 and 81: obtenue à un mois post-opératoire
- Page 84 and 85: L’ostéosarcome intra-médullaire
- Page 87 and 88: Tun Orthop 2008, Vol 1, N° 2Ayadi
- Page 89 and 90: Tun Orthop 2008, Vol 1, N° 2Ayadi
- Page 91 and 92: Tun Orthop 2008, Vol 1, N° 2Mnif H
- Page 93 and 94: Tun Orthop 2008, Vol 1, N° 2Mnif H
- Page 95 and 96: Tun Orthop 2008, Vol 1, N° 2Kandar
- Page 97 and 98: Cas CliniqueTunisie OrThOpédiqueAn
- Page 99 and 100: Tun Orthop 2008, Vol 1, N° 2204Gua
- Page 101 and 102: Cas CliniqueTunisie OrThOpédiqueAn
- Page 103 and 104: Tun Orthop 2008, Vol 1, N° 2208Say
- Page 105 and 106: Quiz Radio-CliniqueTunisie OrThOpé
- Page 107 and 108: Tun Orthop 2008, Vol 1, N° 2Louati
- Page 109 and 110: Articles ImmigrésTunisie OrThOpéd
- Page 111 and 112: Tun Orthop 2008, Vol 1, N° 2Articl
- Page 113 and 114: Tun Orthop 2008, Vol 1, N° 2Articl
- Page 115 and 116: Articles sous MicroscopeTunisie OrT
- Page 117 and 118: Tun Orthop 2008, Vol 1, N° 2222Art
- Page 119 and 120: Tun Orthop 2008, Vol 1, N° 2Articl
- Page 121 and 122: Tun Orthop 2008, Vol 1, N° 2226Art
- Page 123 and 124: Tun Orthop 2008, Vol 1, N° 2Articl
- Page 125: Recommandations aux AuteursTunisie