The Design of Diagnostic Medical Facilities where ... - ResearchGate
The Design of Diagnostic Medical Facilities where ... - ResearchGate
The Design of Diagnostic Medical Facilities where ... - ResearchGate

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
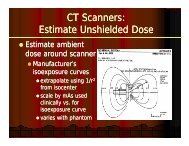
3.1.3 Computed Tomography (CT)<br />
CT allows cross sectional imaging which was traditionally <strong>of</strong> the single ‘snap-shot’ form <strong>of</strong> the head or body.<br />
Modern CT systems produce multiple slices, enable faster three-dimensional imaging, and allow for real-time<br />
tracking <strong>of</strong> events as in fluoroscopy. <strong>The</strong>se systems have greatly enhanced the clinical value <strong>of</strong> CT and also<br />
allow for much more rapid patient scanning. For both reasons the workload in CT rooms has increased and<br />
the radiation levels in the vicinity <strong>of</strong> a CT scanner are possibly higher than for any other imaging modality.<br />
Staff are not generally expected to be in the vicinity <strong>of</strong> the patient during procedures, so the mechanisms <strong>of</strong><br />
radiation protection include the operator screen and the room size approaches already mentioned. However,<br />
the functions accommodated in the operator area are greatly expanded and <strong>of</strong>ten include direction and<br />
analysis <strong>of</strong> the examination by the radiologist as it happens, and observation <strong>of</strong> the results by the referring<br />
clinical team. Thus the operator’s cubicle in effect acquires a consultation, reporting and analysis function<br />
and occupies a considerable area. <strong>The</strong>re is normally a panoramic window and a door from this area to the<br />
CT room.<br />
3.1.4 Shared function rooms<br />
<strong>The</strong>re are an increasing number <strong>of</strong> situations involving rooms with shared functions, one <strong>of</strong> which has a<br />
radiological component. At the extreme upper level <strong>of</strong> this range are operating theatres for vascular<br />
procedures which also have full permanent fixed radiological equipment installed. However, more commonly,<br />
these applications involve low-dose fluoroscopy for short time periods – e.g. during or following orthopaedic<br />
procedures. By comparison with conventional radiological practice, a large number <strong>of</strong> staff may be present<br />
in the room at the time. Because <strong>of</strong> the relatively low doses, radiation protection requirements are generally<br />
less demanding than in the other facilities described above. However the large number <strong>of</strong> staff, not all <strong>of</strong><br />
whom will be trained in radiation protection, presents special problems. In practice a combination <strong>of</strong> mobile<br />
shields, staff withdrawing from the immediate area and limited structural shielding can usually provide a<br />
good solution. However, the design <strong>of</strong> these areas is generally approached on a case by case basis. In<br />
addition, the number and type <strong>of</strong> these areas is increasing, and now routinely includes the Intensive Care,<br />
High Dependency, <strong>The</strong>atre, and Emergency Medicine environments (Section 3.6).<br />
3.2 Some general comments on shielding<br />
From the point <strong>of</strong> view <strong>of</strong> providing shielding at the room boundaries, it is important to weigh up whether<br />
it is more economical to maximise space or install more structural shielding. For example, it may be possible<br />
to designate a relatively large space for an X‐ray room, and as a result <strong>of</strong> the increased distances to the<br />
occupants <strong>of</strong> nearby areas the shielding requirements can be significantly reduced. <strong>The</strong> cost and practical<br />
implications <strong>of</strong> distance versus shielding should be considered in optimising the design solution. This will be<br />
considered further in Chapter 5 and may be particularly important with some newer techniques with very<br />
demanding shielding requirements. From the point <strong>of</strong> view <strong>of</strong> providing for those who must work within the<br />
controlled or supervised areas that coincide with the room boundaries, there are three approaches to<br />
providing protection that impact on room design or equipment specification. <strong>The</strong>se are:<br />
• Fixed screen: This is a screen which attenuates radiation and behind which the operator console and any<br />
other necessary operator control systems (e.g. emergency stop switch) are located. Where the design<br />
allows, the screen should be positioned so that it protects the staff entry door and staff can enter and<br />
16<br />
<strong>The</strong> <strong>Design</strong> <strong>of</strong> <strong>Diagnostic</strong> <strong>Medical</strong> <strong>Facilities</strong> <strong>where</strong> Ionising Radiation is used